De los muchos cambios que experimentan las mujeres al quedarse embarazadas, uno de los más comunes y rápidos en hacer su aparición es la disnea, o lo que es lo mismo la dificultad para respirar y una sensación de cansancio y fatiga al menor movimiento. Una dificultad que no se presenta de forma constante ni siempre con la misma intensidad.
¿De qué depende? Como en todo, de cada embarazada y de cada gestación. Aunque no hay una exactitud milimétrica para definir la disnea en las embarazadas, Juan Luis Delgado, presidente de la Sección de Medicina Perinatal de la SEGO (Sociedad Española de Ginecología y Obstetricia) ha explicado a Ser Padres que esa disnea suele estar relacionada con las adaptaciones anatómicas, bioquímicas y fisiológicas que sufren las futuras madres. Adaptaciones que tienen que ver con el aumento de la progesterona, que afecta al centro respiratorio, y con el aumento del consumo de oxígeno.
No sólo eso. Según recuerda el doctor, las embarazadas también sufren adaptaciones de índole mecánico. Esto se explica con la compensación que la mujer tiene que hacer para mantener el centro de gravedad y con la que el diafragma cambia de posición. También se explica con la restricción de espacio que hay en el tórax al acortarse la caja torácica.
Ahora bien, por molesta que pueda resultar la disnea, cuando ésta tiene que ver con los cambios anteriores no es grave. Otra cosa muy distinta es cuando la disnea tiene un origen patológico que, según matiza Delgado, suele ser cardiopulmonar.
Si te estás preguntando cómo hacer la diferencia entre una disnea de origen anatómico de otra de origen patológico, el experto consultado despeja esa duda al afirmar que “la tos suele ser un signo claro de que la disnea es de origen cardiopulmonar”. Sobre todo, si esa tos es seca, irritativa y empeora por las noches, o si viene acompañada de moco. Sea como sea, lo importante es que si hay tos se consulte con el médico.
Sea como sea, lo importante es que si hay tos se consulte con el médico.
Respecto al momento de aparición de esas dificultades para respirar, Delgado indica que pueden sentirse desde el principio hasta el final del embarazo, aunque no siempre es así. Durante el primer y el segundo trimestre, las disneas suelen ser muy leves o leves y permiten la realización de ejercicio físico. Al final del segundo trimestre y en el tercero, la cosa suele cambiar. ¿Por qué? Porque el aumento significativo del volumen sanguíneo influye en la aparición de la disnea.
Para combatirla, desde el principio y hasta el final de la gestación, Juan Luis Delgado recuerda que es conveniente y muy recomendable evitar dormir boca arriba (en posición decúbito supino). “El útero, al crecer, comprime los grandes vasos abdominales –la aorta y la vena cava- dando lugar a una disminución del retorno venoso (de la sangre) al corazón. Cuando esto ocurre se puede sufrir un síncope (un mareo)”, advierte.
De ahí la importancia de dormir de lado o ligeramente de lado. Si el mareo también llega en esta posición o al hacer ejercicio moderado durante el embarazo, entonces también hay que consultarlo con el médico porque podríamos estar ante un problema cardíaco.
Además de evitar dormir boca arriba, Delgado aconseja que las embarazadas cambien frecuentemente de posición también durante el día. Esto implica mover piernas, espalda y cuerpo y no permanecer sentadas durante largos ratos, además de adaptar en la medida de lo posible la actividad diaria.
Si pese a las prevenciones, la disnea hace su aparición, mientras que sea leve no hay lugar para la alarma ni para la madre ni para el bebé. Y es que según recuerda el experto consultado, “los bebés tienen una fuerte capacidad de adaptación y al igual que la madre son capaces de modular la cantidad de riego sanguíneo que dirigen a cada órgano”.
En caso de que la disnea sea más grave y venga acompañada de tos, Delgado insiste en que la embarazada consulte con su médico quien seguramente la derivará al neumólogo o cardiólogo para determinar dónde está el origen de esas dificultades para respirar, y proceder a su tratamiento.
Sin comentarios
Suscríbete a Bebés y más
Silvia Díaz
@madreaventura
Durante el embarazo, la función respiratoria de la mujer se ve afectada por diversos factores, como la acción de las hormonas y la alteración de la posición del diafragma al aumentar la posición del útero. Esto provoca una sensación de falta de aire y fatiga que se hace más notable en el tercer trimestre.
Te explicamos con detalle por qué se produce esta molestia y cuándo es recomendable consultar con el médico.
A la sensación de falta de aire durante el embarazo se le denomina ‘disnea de la embarazada’, y según la Fundación Argentina de Tórax se calcula que se presenta en un 60-70% de las embarazadas, especialmente antes de la semana 19 y partir de la semana 31 de gestación.
Aunque las causas de la disnea fisiológica durante el embarazo no se conocen con precisión, parece tener que ver con el aumento de la progesterona y una respuesta excesiva de los receptores químicos periféricos y centrales, que inducen una ventilación muy superior a las demandas metabólicas reales.
A menudo también se asocia la falta de aliento a los cambios mecánicos que se producen por la expansión abdominal -especialmente a partir de la segunda mitad del embarazo-, que hace que los músculos respiratorios se debiliten debido a la elevación del diafragma, disminuyendo la capacidad de expansión de la caja torácica.
Es importante mencionar que aunque se trata de un síntoma molesto, la disnea fisiológica de la embarazada no entraña riesgos para la salud del bebé, pues es una molestia leve y pasajera que no repercute en el nivel de oxígeno que le llega a través de la placenta.
La disnea fisiológica en la embarazada sana se produce de forma gradual (es decir, a medida que aumenta el embarazo) y sus síntomas son leves.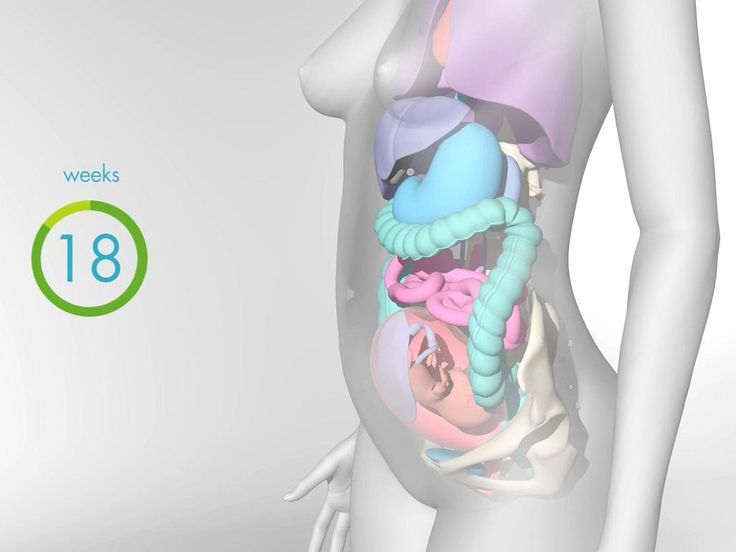 Además, no se manifiestan con la misma intensidad siempre, ni es una sensación constante.
Además, no se manifiestan con la misma intensidad siempre, ni es una sensación constante.
Es muy común que esta falta de aire se presente cuando la embarazada está sentada, pues deja caer su peso sobre el abdomen y esto comprime aún más el diafragma. Pero también es muy probable que sienta que le falta el aliento cuando realiza ejercicio físico durante la última etapa de la gestación, ya que, como hemos visto, el volumen de la tripa puede dificultar la expansión de la caja torácica.
Es importante mencionar que aunque se trata de un síntoma molesto, la disnea fisiológica de la embarazada no entraña riesgos para la salud del bebé, pues es una molestia leve y pasajera que no repercute en el nivel de oxígeno que le llega a través de la placenta.
Aunque se trata de una molestia puntual, si en algún momento sientes que te falta el aire puedes poner en práctica los ejercicios de respiración profunda y consciente que enseñan en los cursos de preparación al parto.
También las técnicas de relajación, cambiar de postura (por ejemplo, levantarte si estás sentada), caminar, descansar y recostarte sobre el lado izquierdo pueden ayudarte a mejorar.
Aunque la disnea fisiológica durante el embarazo es completamente normal y sucede con mucha frecuencia, es recomendable que lo hables con tu médico o matrona para asegurar que todo marcha bien.
Igualmente, es importante diferenciar esta molestia común de otros problemas de salud que podrían presentarse durante el embarazo y que requieren de atención médica urgente.
Así, por ejemplo, si se presentan algunos de estos síntomas asociados a esa “falta de aire” que venimos mencionando, es necesario consultar con el médico:

Fotos | iStock
Compartir
“Estoy embarazada y siento que me falta el aire”: ¿por qué me ocurre y cuándo debo consultar con el médico?
Temas
Spinal neurosurgical pathology and pregnancy
Website of the publishing house “Media Sfera”
contains materials intended exclusively for healthcare professionals. By closing this message, you confirm that you are a registered medical professional or student of a medical educational institution.
By closing this message, you confirm that you are a registered medical professional or student of a medical educational institution.
Androsova Ya.Yu.
GBUZ MO “Moscow Regional Research Institute of Obstetrics and Gynecology” of the Ministry of Health of the Moscow Region
Petrukhin V.A.
GBUZ MO “Moscow Regional Research Institute of Obstetrics and Gynecology” of the Ministry of Health of the Moscow Region
Akhvlediani K.N.
GBUZ MO “Moscow Regional Research Institute of Obstetrics and Gynecology” of the Ministry of Health of the Moscow Region
Lubnin A.Yu.
National Medical Research Center for Neurosurgery named after Academician N.N. Burdenko» of the Ministry of Health of Russia
Petrov P.A.
GBUZ MO “Moscow Regional Research Institute of Obstetrics and Gynecology” of the Ministry of Health of the Moscow Region
Spinal neurosurgical pathology and pregnancy
Authors:
Androsova Ya. Yu., Petrukhin V.A., Akhvlediani K.N., Lubnin A .Yu., Petrov P.A.
Yu., Petrukhin V.A., Akhvlediani K.N., Lubnin A .Yu., Petrov P.A.
More about the authors
Magazine:
Russian Bulletin of an obstetrician-gynecologist. 2022;22(1): 28‑34
DOI:
10.17116/rosakush30222201128
How to quote
Androsova Ya.Yu., Petrukhin V.A., Akhvlediani K.N., Lubnin A.Yu., Petrov P.A.
Spinal neurosurgical pathology and pregnancy. Russian Bulletin of an obstetrician-gynecologist.
2022;22(1):28-34.
Androsova YaYu, Petrukhin VA, Akhvlediani KN, Lubnin AYu, Petrov PA. Spinal neurosurgical pathology and pregnancy. Russian Bulletin of Obstetrician-Gynecologist. 2022;22(1):28‑34. (In Russ.).
https://doi.org/10.17116/rosakush30222201128
Authors:
Androsova Ya.Yu., Petrukhin V.A., Akhvlediani K.N., Lubnin A.Yu., Petrov P.A.
More about the authors
Close metadata
Present-day scientific literature data on the course of pregnancy, delivery tactics in patients with spinal neurosurgical pathology (degenerative-dystrophic diseases of the spine, spinal injury, primary tumors of the spine and spinal cord) are presented.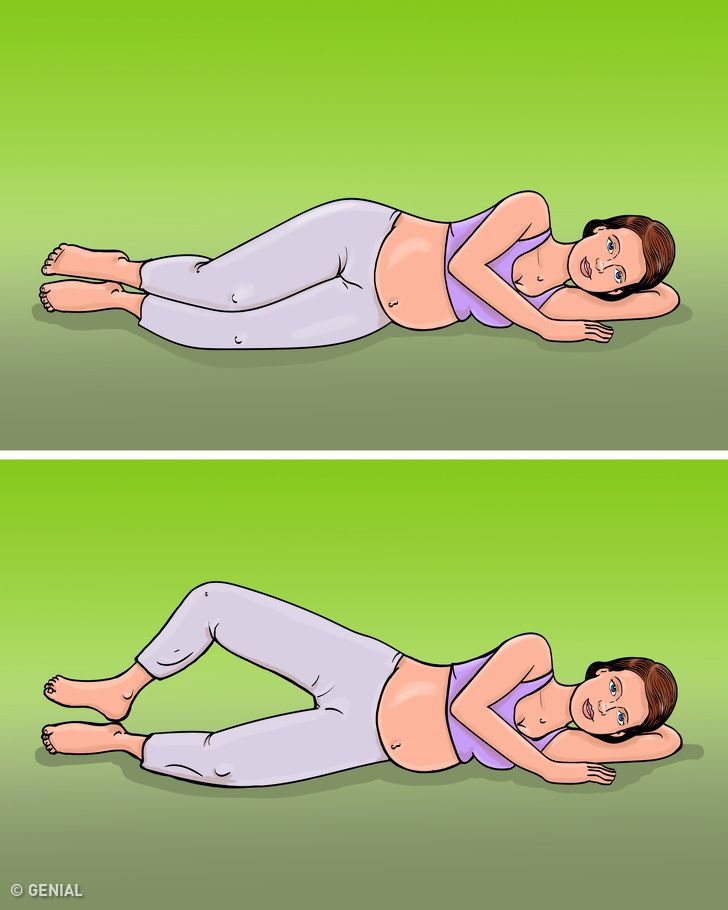 According to the data of domestic and foreign studies in women with spinal neurosurgical pathology, the number of observations of preterm labor, labor anomalies, postpartum complications increases, premature and immature full-term babies are born more often in a state of asphyxia, which leads to an increase in maternal and perinatal morbidity and mortality. Neurosurgical interventions, despite the sufficient prevalence of spinal pathology during pregnancy, are carried out only in cases where, as a result of the rapid progression of neurological symptoms, there is a high risk of disability or a threat to the life of the mother. There are no generally accepted algorithms for managing pregnancy and treating this category of patients.
According to the data of domestic and foreign studies in women with spinal neurosurgical pathology, the number of observations of preterm labor, labor anomalies, postpartum complications increases, premature and immature full-term babies are born more often in a state of asphyxia, which leads to an increase in maternal and perinatal morbidity and mortality. Neurosurgical interventions, despite the sufficient prevalence of spinal pathology during pregnancy, are carried out only in cases where, as a result of the rapid progression of neurological symptoms, there is a high risk of disability or a threat to the life of the mother. There are no generally accepted algorithms for managing pregnancy and treating this category of patients.
Keywords:
pregnancy
spinal pathology
degenerative-dystrophic and dysplastic diseases of the spine
spine and spinal cord injuries
tumors of the spine and spinal cord
Authors:
Androsova Ya. Yu.
Yu.
GBUZ MO “Moscow Regional Research Institute of Obstetrics and Gynecology” of the Ministry of Health of the Moscow Region
Petrukhin V.A.
GBUZ MO “Moscow Regional Research Institute of Obstetrics and Gynecology” of the Ministry of Health of the Moscow Region
Akhvlediani K.N.
GBUZ MO “Moscow Regional Research Institute of Obstetrics and Gynecology” of the Ministry of Health of the Moscow Region
Lubnin A.Yu.
National Medical Research Center for Neurosurgery named after Academician N.N. Burdenko» of the Ministry of Health of Russia
Petrov P.A.
GBUZ MO “Moscow Regional Research Institute of Obstetrics and Gynecology” of the Ministry of Health of the Moscow Region
References:
 Tyumen: Tyumen State University; 2002.
Tyumen: Tyumen State University; 2002. Spine (Phila Pa 1976). 2001;26:13:1449-1456. https://doi.org/10.1097/00007632-200107010-00015
Spine (Phila Pa 1976). 2001;26:13:1449-1456. https://doi.org/10.1097/00007632-200107010-00015  J Phys Ther Sci. 2015;27:1:279-284. https://doi.org/10.1589/jpts.27.279
J Phys Ther Sci. 2015;27:1:279-284. https://doi.org/10.1589/jpts.27.279  Epidural steroids: a comprehensive, evidence-based review. Reg Anesth Pain Med. 2013;38:3:175-200. https://doi.org/10.1097/AAP.0b013e31828ea086
Epidural steroids: a comprehensive, evidence-based review. Reg Anesth Pain Med. 2013;38:3:175-200. https://doi.org/10.1097/AAP.0b013e31828ea086  Assessment of cauda equina syndrome progression pattern to improve diagnosis. Spine. 2014;39:Issue 7:596-602. https://doi.org/10.1097/BRS.0000000000000079
Assessment of cauda equina syndrome progression pattern to improve diagnosis. Spine. 2014;39:Issue 7:596-602. https://doi.org/10.1097/BRS.0000000000000079  org/10.1111/1552-6909.12200
org/10.1111/1552-6909.12200  2007.09.025
2007.09.025  1159/000488756
1159/000488756  Yu., Konovalov N.A., Shmigelsky A.V., Tabassaranskiy T.F., Avkhlediani K.N., Savin I.A., Onoprienko R.A., Martynova M.A. Acute spinal catastrophe caused by a benign mass formation of the spinal cord in a pregnant woman. Bulletin of Intensive Care. 2016;1:50-57.
Yu., Konovalov N.A., Shmigelsky A.V., Tabassaranskiy T.F., Avkhlediani K.N., Savin I.A., Onoprienko R.A., Martynova M.A. Acute spinal catastrophe caused by a benign mass formation of the spinal cord in a pregnant woman. Bulletin of Intensive Care. 2016;1:50-57.  Fetal magnetic resonance imaging: jumping from 1.5 to 3 tesla (preliminary experience). Pediatric Radiol. 2014;44:4:376-386; quiz 373-375. https://doi.org/10.1007/s00247-013-2857-0
Fetal magnetic resonance imaging: jumping from 1.5 to 3 tesla (preliminary experience). Pediatric Radiol. 2014;44:4:376-386; quiz 373-375. https://doi.org/10.1007/s00247-013-2857-0 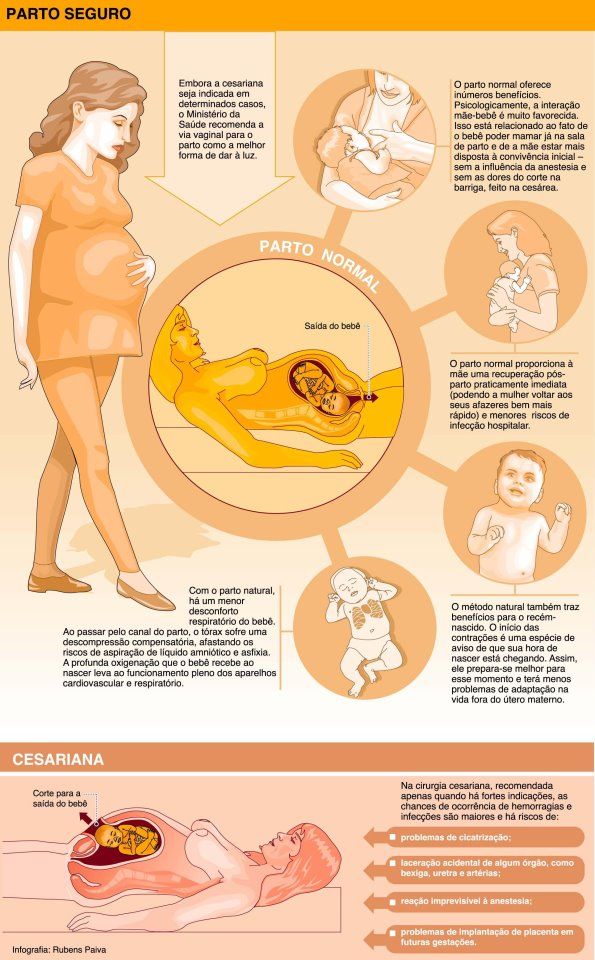 org/10.1002/jmri.24011
org/10.1002/jmri.24011  Anaesthesia for spinal tumor in the pregnant patient: a case report. J Anesth Crit Care Open Access. 2017;8:6:00324. https://doi.org/10.15406/jaccoa.2017.08.00324
Anaesthesia for spinal tumor in the pregnant patient: a case report. J Anesth Crit Care Open Access. 2017;8:6:00324. https://doi.org/10.15406/jaccoa.2017.08.00324 Close metadata
The Republican Children’s Clinical Hospital of the Ministry of Health of the Udmurt Republic uses cookies to improve the convenience of working with the site. The cookie contains data about past visits to the site. If you do not want this data to be processed, disable cookies in your browser settings.
home
Prevention of mechanical asphyxia
in infants
(memo for parents)
Mechanical asphyxia (suffocation) – holding the breath for more than 20 seconds. due to mechanical obstruction (compression of the neck, chest, abdomen), closure of the airway lumen with mucus, food, soft or hard objects. It is accompanied by a violation of well-being, a change in skin color (cyanosis or pallor), a pronounced sharp decrease in muscle tone, and lethargy. May cause the death of a child.
May cause the death of a child.
Causes of mechanical asphyxia
1. Covering the child’s airways with a soft object (pillow, toy).
2. Covering the airways with the mother’s breast during feeding.
3. Ingress of foreign bodies into the respiratory tract (small toys, buttons, rings, coins, etc.).
4. Puffing and getting milk not into the child’s esophagus, but into the larynx, sometimes the bronchi.
5. Frequent regurgitation.
6. Compression of the neck area with chains with crosses (talismans), braid with a pacifier.
Prophylaxis of mechanical asphyxia
1. After each feeding, hold the baby vertically with a “column”. Frequent and profuse regurgitation is a reason to see a doctor.
2. Always turn the head of a lying baby on its side, the lower handle is “free”.
3.Do not put the baby on the pillow.
4. Do not put the baby on a soft feather bed.