Hoy te voy a hablar de la herida de cesárea. Un parto puede terminar en parto vaginal o en cesárea. Tan normal es una como otra terminación. Piensa que entre el 20 y 35% de los partos (según los hospitales) termina en la realización de una cesárea.
En otros artículos, te he hablado sobre cómo transcurren las primeras horas tras una cesárea en el hospital (quirófano, sala de recuperación de la anestesia y planta), te he respondido a las preguntas más frecuentes tras una cesárea que me suelen hacer mís pacientes.
La infección de la herida quirúrgica es una de las complicaciones más frecuentes en la cirugía. En concreto, las infecciones de la herida en las cesáreas suele ser del 5%.
Esta frecuencia justifica que le dediquemos el artículo de hoy. Por otro lado, cuándo acabas de tener a tu bebé, te notarás absolutamente agotada. Estás cansada, agotada del esfuerzo y de no dormir cuidando a tu bebé. Cualquier pequeña complicación parece una montaña insuperable.
Con el artículo de hoy quiero ayudarte y facilitarte la situación. Si aparece cualquiera de los síntomas que te comento, acude a tu médico/matrona/ginecólogo.
En este artículo quiero llamar tu atención sobre dos puntos fundamentales:
Existen varios problemas durante la gestación que pueden aumentar tu riesgo. La diabetes gestacional es uno de ellos. Mi consejo es extremar los controles para mantener los niveles de azúcar en sangre dentro de los niveles de normalidad.
Si has tenido problemas de desnutrición (nivel socioeconómico bajo o tercer mundo) obviamente tus defensas son menos eficaces.
Las pacientes que padecen enfermedades con tendencia a la inmunosupresión.
El origen o la causa de la cesárea también influye. Si previamente tenías infección en la bolsa amniótica (corioamnionitis) o fiebre antes o durante el parto.
La obesidad aumenta mucho el riesgo. Tener excesiva grasa en la pared abdominal favorece enormemente la infección posterior de la herida.
Los partos prolongados, de muchas horas, que obligan a realizar muchas exploraciones vaginales son también factores de riesgo. Todo influye en que la tasa de complicaciones infecciosas en las cesárea urgentes intraparto sea mayor que cuando la cesárea es programada (no urgente).
Tras ver los factores que te he comentados, ya sospecharás que los gérmenes pueden venir la propia piel o desde el canal del parto y bolsa amniótica.
Tras la cesarea y durante los primeros días en el hospital aprenderás a cuidar la herida de forma correcta. No es necesario hacer nada especial. Simplemente observa cómo la enfermera o tu médico en el hospital realizan las curas diarias y los lavados de la herida.
No es necesario hacer nada especial. Simplemente observa cómo la enfermera o tu médico en el hospital realizan las curas diarias y los lavados de la herida.
Las heridas no se infectan el primer día. Suelen aparecer síntomas entre el 2º-7º día. Es decir en muchas ocasiones ya estás en casa cuando notas los primeros síntomas.
A nivel local el síntoma principal es el enrojecimiento de la piel alrededor de una parte de la herida. En ocasiones puedes notar una induración (zona más tensa dura, enrojecida y algo sobrellevada).
La aparición de secreción, sobre todo purulenta, es motivo de consulta obligada a tú médico.
Por supuesto, si aparece fiebre tras el parto, consulta a tu médico. En estos casos la exploración de la herida de la cesárea y de las mamas para descartar una mastitis son necesarias.
Por tanto, estos son los tres síntomas principales: enrojecimiento, fiebre y secreción por la herida.
Si el diagnostico está claro, con los síntomas anteriores, ya podemos pasar al tratamiento.
En ocasiones puede ser aconsejable hacer alguna otra prueba como analíticas de sangre o cultivo de la herida.
El tomar una cultivo de la secreción de la herida es muy sencillo. Basta con pasar un hisopeo de algodón o bastoncillo y mojarlo en la secreción de la herida. Se envía al laboratorio y no informa sobre el germen exacto que produce la infección y sobre los antibióticos más adecuado.
El problema es que el resultado tarda unos cuantos días y no podemos demorar el tratamiento.
Hecho el diagnóstico, ponemos tratamiento en el mismo momento.
Lo más importante es el lavado de la herida. Para ello es necesario quitar alguna grapa (o punto, según el caso) y abrir la parte de la herida que esté infectada para que salga la secreción (drenaje).
Posteriormente, seguimos con el lavado abundante con suero fisiológico.
Elimaremos los restos de tejido necrótico y esfacelos, coágulos y serenidad. La herida debe de quedar lo más limpia posible (desbridamiento).
En algunas ocasiones, podemos emplear algún tipo de antiséptico para profundizar en la limpieza tipo clorhexidina.
Es importante ser constantes. Haremos la limpieza una o dos veces al día, según la gravedad.
Si la infección es pequeña, en pocos días se controla la infección, pero si es extensa nos obliga a abrir completamente la herida, ir curándola poco a poco, y dejar que posteriormente vaya cerrando de forma espontánea en las semanas siguientes.
Cada caso (cada mujer) es diferente.
Tu médico decidirá si además necesitas tomar antibióticos orales para ayudar en la desinfección.
La infección de la herida de cesárea no debe ser un motivo de agobio, pues ya tienes bastante preocupación con el cuidado de tú bebé.
Extrema los cuidados, sobre todo si tienes factores de riesgo, para evitar que la herida se infecte.
En caso de haberse infectado, sigue las indicaciones de tu médico y en pocos días todo se habrá quedado en la anécdota.
Cochrane Evidence Synthesis and Methods ►
Las mujeres a las que se les realiza una cesárea tienen de cinco a 20 veces más probabilidades de presentar una infección, en comparación con las mujeres que tienen un parto vaginal. Estas infecciones se pueden presentar en los órganos dentro de la pelvis, alrededor de la incisión quirúrgica y a veces en la orina. Las infecciones pueden ser graves y en muy pocas ocasiones pueden provocar la muerte materna. Los posibles efectos beneficiosos de la reducción de la infección para la madre se deben equilibrar con cualquier efecto adverso como náuseas, vómitos, erupción cutánea y, pocas veces, reacciones alérgicas en la madre, así como con cualquier efecto de los antibióticos sobre el recién nacido, incluido el muguet. Esta revisión analizó si los antibióticos son efectivos para prevenir la infección en las mujeres que se someten a una cesárea. También examinó el efecto de proporcionar antibióticos antes o después de pinzar el cordón y diferentes tipos de antibióticos. La revisión encontró 95 estudios que incluyeron más de 15 000 mujeres. El uso sistemático de antibióticos en la cesárea redujo el riesgo de infecciones de la herida y el útero en las madres, así como el riesgo de complicaciones graves de infecciones para las madres en el 60% al 70%. Esta reducción ocurrió cuando la cesárea fue electiva o de urgencia, y cuando los antibióticos se administraron antes o después del pinzamiento del cordón umbilical. La evidencia que apoyó el tratamiento con antibióticos fue de calidad moderada, pero a menudo no se describió suficientemente bien la forma en la que se realizó el estudio. Ninguno de los estudios analizó adecuadamente los posibles efectos adversos sobre el recién nacido y, por lo tanto, aunque hay efectos beneficiosos para la madre, existe cierta incertidumbre sobre si hay efectos importantes sobre el recién nacido.
Esta revisión analizó si los antibióticos son efectivos para prevenir la infección en las mujeres que se someten a una cesárea. También examinó el efecto de proporcionar antibióticos antes o después de pinzar el cordón y diferentes tipos de antibióticos. La revisión encontró 95 estudios que incluyeron más de 15 000 mujeres. El uso sistemático de antibióticos en la cesárea redujo el riesgo de infecciones de la herida y el útero en las madres, así como el riesgo de complicaciones graves de infecciones para las madres en el 60% al 70%. Esta reducción ocurrió cuando la cesárea fue electiva o de urgencia, y cuando los antibióticos se administraron antes o después del pinzamiento del cordón umbilical. La evidencia que apoyó el tratamiento con antibióticos fue de calidad moderada, pero a menudo no se describió suficientemente bien la forma en la que se realizó el estudio. Ninguno de los estudios analizó adecuadamente los posibles efectos adversos sobre el recién nacido y, por lo tanto, aunque hay efectos beneficiosos para la madre, existe cierta incertidumbre sobre si hay efectos importantes sobre el recién nacido.
Conclusiones de los autores:
Las conclusiones de esta revisión apoyan la recomendación de que se deben administrar antibióticos profilácticos de forma sistemática todas las mujeres que se someten a una cesárea para prevenir la infección. En comparación con placebo o ningún tratamiento, la administración de antibióticos profilácticos a las mujeres sometidas a cesárea redujo la incidencia de infección de la herida, la endometritis y las complicaciones infecciosas graves entre el 60% y el 70%. Hubo pocos datos sobre los efectos adversos y ninguna información del efecto de los antibióticos sobre el recién nacido, lo que dificultó la evaluación de los efectos beneficiosos y perjudiciales en general. Los antibióticos profilácticos administrados a todas las mujeres a las que se les realizó cesárea electiva o no electiva son claramente beneficiosos para las mujeres, pero existe incertidumbre acerca de las consecuencias para los recién nacidos.
Leer el resumen completo…
Antecedentes:
El factor de riesgo único más importante para la infección materna posparto es la cesárea. Aunque las guías respaldan el uso de antibióticos profilácticos para las mujeres que se someten a una cesárea, no hay una aplicación uniforme de esta recomendación. Esta es una actualización de una revisión Cochrane publicada por primera vez en 1995 y actualizada por última vez en 2010.
Aunque las guías respaldan el uso de antibióticos profilácticos para las mujeres que se someten a una cesárea, no hay una aplicación uniforme de esta recomendación. Esta es una actualización de una revisión Cochrane publicada por primera vez en 1995 y actualizada por última vez en 2010.
Objetivos:
Evaluar los efectos de los antibióticos profilácticos comparados con ningún antibiótico profiláctico sobre las complicaciones infecciosas en mujeres a las que se les realiza una cesárea.
Métodos de búsqueda:
Se hicieron búsquedas en el registro de ensayos del Grupo Cochrane de Embarazo y Parto (Cochrane Pregnancy and Childbirth Group) (31 de julio 2014) y en las listas de referencias de los estudios recuperados.
Criterios de selección:
Ensayos controlados aleatorizados (ECA) y cuasialeatorizados que compararon los efectos de los antibióticos profilácticos versus ningún tratamiento en mujeres a las que se les realiza una cesárea.
Obtención y análisis de los datos:
Dos autores de la revisión de forma independiente evaluaron los estudios para la inclusión, evaluaron el riesgo de sesgo y realizaron la extracción de los datos. Los resultados primarios de importancia clínica fueron la infección de la herida, la endometritis, las complicaciones infecciosas graves de la madre y los efectos adversos en el recién nacido. Los datos dicotómicos se presentaron como riesgo relativo (RR), con intervalos de confianza (IC) del 95% y los ensayos se combinaron en metanálisis. Se evaluó la calidad de la evidencia mediante el enfoque GRADE.
Los resultados primarios de importancia clínica fueron la infección de la herida, la endometritis, las complicaciones infecciosas graves de la madre y los efectos adversos en el recién nacido. Los datos dicotómicos se presentaron como riesgo relativo (RR), con intervalos de confianza (IC) del 95% y los ensayos se combinaron en metanálisis. Se evaluó la calidad de la evidencia mediante el enfoque GRADE.
Resultados principales:
Se identificaron 95 estudios que reclutaron más de 15 000 mujeres. En comparación con placebo o ningún tratamiento, la administración de antibióticos profilácticos en las mujeres sometidas a cesárea redujo la incidencia de infección de la herida (RR 0,40; IC del 95%: 0,35 a 0,46, 82 estudios, 14 407 mujeres), la endometritis (RR 0,38; IC del 95%: 0,34 a 0,42, 83 estudios, 13 548 mujeres) y las complicaciones infecciosas graves maternas (RR 0,31; IC del 95%: 0,20 a 0,49, 32 estudios, 6159 mujeres). Cuando solo se analizaron los estudios que incluyeron mujeres sometidas a una cesárea electiva, también se observó una reducción de la incidencia de infecciones de la herida (RR 0,62; IC del 95%: 0,47 a 0,82; 17 estudios, 3537 mujeres) y de endometritis (RR 0,38; IC del 95%: 0,24 a 0,61; 15 estudios, 2502 mujeres) con los antibióticos profilácticos. Se observaron estimaciones similares de los efectos si los antibióticos se administraron antes o después de pinzar el cordón. Se estudió el efecto de diferentes regímenes de antibióticos y se observaron reducciones similares en la incidencia de infecciones con la mayoría de los antibióticos y combinaciones.
Se observaron estimaciones similares de los efectos si los antibióticos se administraron antes o después de pinzar el cordón. Se estudió el efecto de diferentes regímenes de antibióticos y se observaron reducciones similares en la incidencia de infecciones con la mayoría de los antibióticos y combinaciones.
No hubo datos disponibles para calcular el efecto de la administración de antibióticos a la madre sobre los resultados del recién nacido. No hay estudios que recopilen e informen de manera sistemática los resultados adversos sobre los recién nacidos, ni sobre el efecto de los antibióticos en el sistema inmunológico de los recién nacidos en desarrollo. Ningún estudio informó sobre la incidencia de la candidiasis oral (muguet) en los recién nacidos. También se describieron en muy pocas ocasiones los efectos adversos maternos.
Se consideró que la evidencia del tratamiento con antibióticos, comparado con ningún tratamiento, fue de calidad moderada; la mayoría de los estudios carecieron de una descripción adecuada de los métodos y se evaluaron como riesgo incierto sesgo.
Notas de traducción:
La traducción y edición de las revisiones Cochrane han sido realizadas bajo la responsabilidad del Centro Cochrane Iberoamericano, gracias a la suscripción efectuada por el Ministerio de Sanidad, Servicios Sociales e Igualdad del Gobierno español. Si detecta algún problema con la traducción, por favor, contacte con Infoglobal Suport, [email protected].
Description
The number of births by caesarean section increases every year and reaches about 40%, so women are more likely to deal with the problem of an inconsistent (thinned) scar on the uterus. The main cause of scar failure is chronic sluggish metroendometritis, the main symptoms are prolonged postmenstrual spotting and pain in the lower abdomen.
Diagnosis of an incompetent scar on the uterus at the stage of pregnancy planning is especially difficult, since it is difficult to make a correct diagnosis only on the basis of ultrasound results. Therefore, the WMT clinic uses the entire range of diagnostic measures to clarify the diagnosis:
Therefore, the WMT clinic uses the entire range of diagnostic measures to clarify the diagnosis:

When the diagnosis of an incompetent scar on the uterus is confirmed at the stage of preconception preparation, the surgeons of the WMT clinic perform a reconstructive plastic surgery – metroplasty. The operation can be performed by laparotomy (open), laparoscopic and vaginal access. Preference is given to laparoscopic access. During surgical intervention, economical excision of the connective tissue scar and layer-by-layer restoration of the uterine wall are performed.
Indications for surgical treatment:
Assessment of the consistency of the scar after metroplasty is carried out after 1, 3, 6 and 12 months using ultrasound. Only after receiving data on the satisfactory condition of the scar, you can plan a pregnancy.
Only after receiving data on the satisfactory condition of the scar, you can plan a pregnancy.
BOOK YOUR APPOINTMENT
Make an appointment with the gynecologist at the WMT clinic by calling 8 (861) 206-03-03 . or leave a request on the site.
Appointment
1. Abramchenko V.V., Bashmakova M.A., Korkhov V.V. Antibiotics in obstetrics and gynecology // St. Petersburg, 2000, 218 p.
Petersburg, 2000, 218 p.
2. Abramchenko V.V., Lantsev E.A. Caesarean section // St. Petersburg, “Medicine”, 1991, 147 p.
3. Avdeev Yu.V. Clinical and microbiological features of endometritis after caesarean section // Midwife. and gin., No. 8.1987, p. 52-55.
4. Avdeev Yu.V. Prediction and early diagnosis of purulent-septic complications, their prevention and treatment after delivery by caesarean section. Candidate of medical sciences diss. // 1985, Ryazan.
5. Ailamazyan E.K., Karpov O.I., Kucherenko M.A. and others. Cefepime as a means of preventing infectious complications during caesarean section in risk groups // Journal of Obstetrics and Women’s Diseases, t.XLVIII, 1999, no. 4.
6. Obstetric and gynecological care. // Ed. V.I. Kulakova, M., 2000, 507 p.
7. Ananiev V.A. The results of caesarean section when applying a single-row and double-row suture to the uterus. // midwife. and gin., 2000, No. 4, p. 26-29.
8. Anisimova M. I., Perepelitsa S.E. et al. Risk of peritonitis after caesarean section // Obstetrics. and gin., No. 3, 1989, p. 42-44.
I., Perepelitsa S.E. et al. Risk of peritonitis after caesarean section // Obstetrics. and gin., No. 3, 1989, p. 42-44.
9. Astsaturova O.R. Diagnosis and treatment of vulvovaginal and chlamydial infections in the third trimester of pregnancy. Diss. candidate of medical sciences // M., 1998, 140 p.
10. Yu.Akhtamova Z.M. The value of microbiological studies in optimizing antibiotic prophylaxis for caesarean section in women with hypochromic anemia. Vestnik ros. ass. Obstetrics and Gynecology, No. 3, Sept. 1996, p. 62-63.
11. P.Akhtamova Z.M. On the place and significance of preventive antibiotic therapy in operative obstetrics // Bulletin of a general practitioner, 1997, No. 1, p. 62-66.1.l
12. Baev O.P. Modern principles of complex prevention, diagnosis and differentiated treatment of purulent-septic complications of caesarean section. Diss. .doc.med.sci. // M., 1998, 325 p.
13. Baev O.R., Strizhakov A.N. Resident flora of the genital tract and the etiology of infectious complications of pregnancy and the postpartum period. and gin., 1997, no. 6, p. 3-7.
and gin., 1997, no. 6, p. 3-7.
14. Baev O.R., Strizhakov A.N. Modern approaches to the prevention of purulent-septic complications after caesarean section. Vestnik ros. ass. Obstetrics and Gynecology, No. 4, Oct. 1997, p. 40-47.
15. Belousova T.I., Bakuleva L.P., Nesterova A.A. Galetsky P.K. Microbiological criteria for predicting postpartum purulent-septic complications // Vopr. och. mat. det., 1988, No. 4, p. 22-25.
16. Burduli G.M. Reproductive losses: causes, risk factors, ways of prevention. //Author. diss. . doc.med. Sciences, M., 1998, 47 p.
17. Buyanova S.N., Senchakova T.N. Diagnosis, treatment and prevention of delayed complications of caesarean section. Vestnik ros. ass. Obstetrics and Gynecology, No. 1, Jan. 1997, p. 65-68.
18. Voropaeva S.D., Sokolova I.E., Emelyanova A.I., Kochieva S.K. The role of non-spore-forming anaerobes in the occurrence of postpartum endometritis. and gin., 1986 No. 8, p. 27-30.
19. Vybornova I.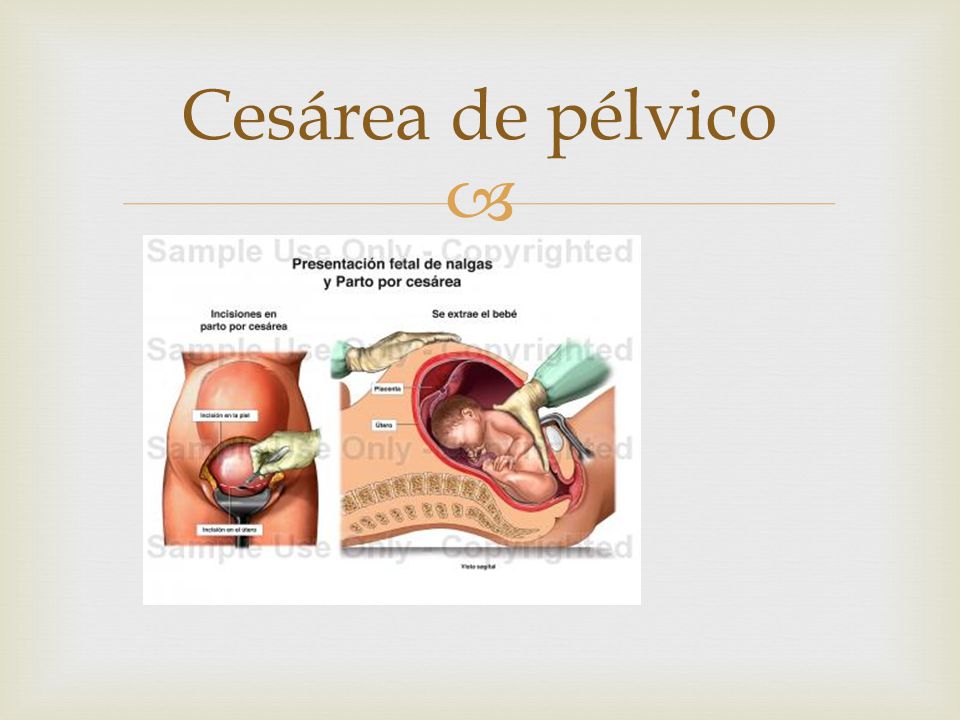 A. Early diagnosis, prevention and treatment of endometritis after caesarean section. // Abstract. diss. Candidate of Medical Sciences, Smolensk, 1998, 19 p.
A. Early diagnosis, prevention and treatment of endometritis after caesarean section. // Abstract. diss. Candidate of Medical Sciences, Smolensk, 1998, 19 p.
20. Gasparyan S.A. Prevention of purulent-inflammatory complications after caesarean section. Diss. . cand. honey. Sciences // Stavropol, 1990, 184 p.
21. Gimpel V.F., Silyava V.P., Kasko L.G1. Efficiency of cefotetan for the prevention of purulent-septic complications after cesarean section. // on Sat. Topical issues of obstetrics and gynecology, Minsk, 1998, p. 22-23.
22. Gromova A.JI. Clinical and experimental substantiation of the use of biofil suture material during caesarean section. // Auto-ref. diss. . Candidate of Medical Sciences, Smolensk, 2000, 17 p.
23. Gurtovoy B.L. Principles of antibacterial prophylaxis and therapy of infectious complications of caesarean section // Congress of the Russian Association of Obstetricians and Gynecologists, 1st. M., 1995, p. 32-33.
24. Gurtovoy B. L., Kulakov V.I., Voropaeva S.D. The use of antibiotics in obstetrics and gynecology. // M., 1996, 140 p.
L., Kulakov V.I., Voropaeva S.D. The use of antibiotics in obstetrics and gynecology. // M., 1996, 140 p.
25. Gurtovoy B.L., Serov V.N., Makatsaria A.D. Purulent-septic diseases in obstetrics. // M., 1981, 255 p.
26. Dobrovolskaya I.A. Prediction of purulent-septic postpartum complications in terms of nonspecific resistance of the pregnant woman’s organism. Midwife. and gin., 1988, no. 9, p. 18-20.
27. Egiev V.N. Suture materials in surgery and gynecology. // Bulletin grew. ass. obstetrics and gynecology, 1995, No. 3, p. 72-75.
28. Zharov E.V. Complex prevention and treatment of purulent-septic complications of caesarean section. Diss. . doc. honey. Sciences // M., 1989, 348 p.
29. Ivanova T.P. Comprehensive prevention of endometritis after caesarean section. Diss. . cand. honey. Sciences // Smolensk, 1998, 120 p.
30. Ivanyan A.N. Purulent-septic diseases in obstetrics and gynecology (early diagnosis, prevention and therapy) // Abstract of the thesis. . diss. cand. honey. Sciences, M., 1994.48 s.
. diss. cand. honey. Sciences, M., 1994.48 s.
31. Karaulov A.V. Augmentin: implementation of the principles of rational antibiotic therapy // Practitioner, 1996, vol. 2, no. 4, p. 46-47.
32. Cesarean section // M., Tehlit, 1997, ed. V.I. Krasnopolsky, 285 p.
33. Kira E.F. Infections and reproductive health // in Sat. “Modern methods of diagnosis, therapy and prevention of STIs and other urogenital infections”, 1999-2000, p. 22-25.
34. Komissarova L.M. Caesarean section and its role in reducing maternal and perinatal pathology. Diss. .doc medical sciences // M., 1998, 82 p.
35. Komissarova J1.M., Galstyan A.A. Preventive antibiotic prophylaxis for caesarean section // Midwife. and gin., 1987, No. 8, p. 7-10.
36. Komissarova JI.M., Chernukha E.A., Puchko T.K. Optimization of caesarean section. // midwife. and gin., 2000, No. 1, p. 14-16.
37. Korshunov V.M., Volodin N.N., Efimov B.A. and other Microecology of the vagina. Correction of microflora in vaginal dysbacteriosis. // M., 1999, 80 p.
// M., 1999, 80 p.
38. Krasnopolsky V.I., Levashova I.I., Zyryaeva N.V., Mareeva L.S. Some problems and prospects for improving the outcomes of caesarean section // Midwife. and gin., No. 3, 1989, p. 18-21.
39. Kulakov V.I., Proshina I.V. Emergency delivery // M., “Medicine”, 1994, 272 p.
40. Kulakov V.I., Ankirskaya A.S., Akopyan T.E., Fursova S.A., Nikonov A.P. Plivasept-antiseptic emulsion for the prevention of endometritis after caesarean section in pregnant women with bacterial vaginosis. // midwife. and gin., 1996, No. 5, p. 51-54.
41. Kulakov V.I., Voropaeva S.D., Ankirskaya A.S. Obligate anaerobic microorganisms in obstetric and gynecological pathology. Vestnik Ros. acad. honey. Sciences, 1996, no. 2, p. 26-29.
42. Kulakov V.I., Karimov Z.D. A method for restoring the lower segment of the uterus in one row during a caesarean section. // midwife. and gin., 1994, No. 1, p. 25-28.
43. Kulakov V.I., Chernukha E.A. The results of caesarean section depending on the method of suturing the uterus and suture material. and gin., 1997, No. 4, p. 18-21.
and gin., 1997, No. 4, p. 18-21.
44. Kulakov V.I., Chernukha E.A., Komissarova L.M. C-section. // M., 1998, 190 p.
45. Kulinich S.I., Trusov Yu.V. and others. Modern features of postpartum endometritis. // Bulletin grew. ass. Obstetrics and Gynecology, No. 1, Jan. 1999, p. 47-51.
46. Lebedev V.A. Caesarean section in modern obstetrics: prevention of maternal and perinatal morbidity and mortality. // Autoref. diss. . doc. honey. Sciences, M., 1999.61 p.
47. Logutova L.S. Optimization of caesarean section. Medical and social aspects.// M., 1996, Author. dis. doc. honey. Sciences, 48 p.
48. Manukhin I.B., Ryzhkov V.V., Fedosova G.N. Prevention of reproductive losses. // Stavropol, 1999, 239 p.
49. Mareeva L.S., Levashova I.I., Ishchenko A.I. and others. Some aspects of surgical tactics of abdominal delivery. // midwife. and gin., 1992, No. 8-12, p. 27-29.
50. Medicine. News bulletin. Medical preparations, equipment, services. // M., August 14, 2001, No. 33, 380 p.
// M., August 14, 2001, No. 33, 380 p.
51. Mirov I.M. C-section. // Ryazan, 1991, 90 p.
52. Mirov I.M. Prediction, early detection, treatment and complex prevention of purulent-inflammatory diseases after childbirth and caesarean section. Dis. . doc. honey. Sciences // Ryazan, 1995, 308 p.
53. Mirov I.M. Perioperative use of antibiotics for caesarean section in parturient women with a high risk of infectious complications. Vestnik ros. ass. Obstetrics and Gynecology, No. 1.1994, p. 65-69.
54. Navashin S.M., Fomina I.P. Rational antibiotic therapy.// M., 1982,495 p.
55. Naumov Yu.G. Regional lymphotropic administration of protease inhibitors in the prevention of purulent-septic complications after cesarean section. // midwife. and gin., 1993, No. 6, p. 22-24.
56. Nikonov A.P. Postpartum endometritis as a manifestation of wound infection (pathogenesis, principles of diagnosis and rational therapy). Diss. .doc honey. Sciences//M., 1993, 318 p.
57. Nikonov A.P., Gurtovoi B.L., Litovsky Yu.R., Ankirskaya A.S. Partial divergence of sutures on the uterus after cesarean section (diagnosis and treatment tactics) // Obstetrician. and gin., 1991, no. 12, p. 30-33.
58. Common infections // Ed. Keita L.G., Bergera G.S., M., 1988, v. 1, 400 p.
59. Omelyanovsky V.V., Buyanova S.N., Shchukina N.A. Basic principles of antibiotic prophylaxis in gynecology // Vestnik ros. ass. Obstetrics and Gynecology, No. 3, 1999, p. 90-94.
60. Puchkov K.V., Gausman B.Ya., Shvalb A.P. The choice of suture material in operative gynecology. Comparative evaluation: biosin, polysorb, vicryl, catgut // Vestnik ros. ass. Obstetrics and Gynecology, No. 1, 1997, p. 83-86.
61. Guidelines for the protection of reproductive health // M., “Triada-X”, 2001, 565 p.
62. Rybin M.V. Immediate and long-term results of a new modification of the caesarean section. Diss. honey. Sciences // M., 1997, 138 p.
63. Salva A. S. Clinic and treatment of endometritis after caesarean section. Diss. . cand. honey. Sciences//M., 1995, 112 p.
64. Serov V.N., Zharov E.V., Makatsaria A.D. Obstetric peritonitis // M., Kron-press, 1997, 251 p.
65. Sidorova I.S., Botvin M.A., Makarov I.O. Prevention of insolvency of the suture on the uterus after cesarean section. // midwife. and gin., 1989, no. 3, p. 30-33
66. Smekuna F.A. Early diagnosis and optimization of the treatment of postpartum infectious diseases in modern conditions. Diss. .doc. honey. Sciences // M., 1988, 329 p.
67. Smekuna F.A., Tumanova V.A., Zak I.R. Prevention of endometritis after cesarean section. and gin., 1991, No. 10, p. 10-13.
68. Improvement of caesarean section and prevention of its complications // Ed. A.N. Strizhakova: Method, recommendations, M., 1996, 27 p.
69. Starostina T.A., Frolova O.G. Mortality after caesarean section // Obstetrics. and gin., 1989, No. 3, p. 22-24.
70. Strizhakov A. N., Baev O.R. Clinical and instrumental assessment of the state of the suture on the uterus and the choice of therapeutic tactics for purulent-septic complications after cesarean section. // midwife. and gin., 1999, No. 5, p. 2127.
71. Strizhakov A.N., Lebedev V.A. Caesarean section in modern obstetrics // M., “Medicine”, 1998, 303 p.
72. Tyutyunnik V.L., Gurtovoy B.L. Prevention and treatment of endometritis after cesarean section // Russian Medical Journal, 2002, v. 10, No. 18 (162), p. 803-805.
73. Filonov S.M. The outcome of caesarean section operations depending on the method of suturing the uterus and suture material. Diss. cand. honey. Sciences // M., 1997, 133 p.
74. Frolova O.G., Nikolaeva E.I., Tokova 3.3. Medico-social aspects of maternal and newborn health. // midwife. and gin., 1994, No. 4, p. 34-37.
75. Tsvelev Yu.V., Kira E.F., Kocherovets V.I., Baskakov V.P. Anaerobic infection in the obstetric and gynecological clinic // St. Petersburg, “Peter”, 1995, p. 313.
76. Chernukha E.A. Generic block // M., Triada-X, 1998, 533 p.
77. Chernukha E.A. Cesarean section present and future // Midwife. and gin., 1997, No. 5, p. 22-28.
78. Yakovlev S.V. The value of cephalosporin antibiotics in the treatment of bacterial infections in the hospital. // Infections and antimicrobial therapy, 2000, vol. 2, no. 3, p. 83-88.
79. Adair C.D., Ernest J.M., Sanchez-Ramos L. et al. Meconium-stained amniotic fluid-associated infectious morbidity: a randomized, double-blind trial of ampicillin-sulbactam prophylaxis // Obst. Gyn., 1996, v. 88, no. 2, p. 216220.
80. Andrews W.W., Shah S.R., Goldenberg R.L. et al. Association of postcesarean delivery endometritis with colonization of the chorioamnion by Ureaplasma urealyticum // Obstet. Gynecol., 1995, v. 85, no. 4, p. 509-514.
81. Atkinson M.W. Owen J., Wren A., Hauth J.C. The effect of manual removal of the placenta on post-cesarean endometritis // Obstet. Gynecol. , 1996, v. 87, no. 1, p. 99-102.
82. Berenson A., Hammil H., Martens M., Faro S. Bacteriologic findings of post-cesarean endometritis in adolescents // Obstet. Gynecol., 1990, v. 75, no. 4, p. 627-629.
83. Berkly A.S., Hirsch J.C., Freedman K.S., Ledger W.J. Cefotaxime for cesarean section prophylaxis in labor intravenous administration vs lavage // J. Reprod. Med., 1990, v. 35, no. 3, p. 214-218.
84. Bibi M., Megdiche H., Ghanem H., Sfaxi I., Nouira M. et al. L’antibiopro-phylaxie dans les cesariennes a priori sans “haut risque infectieux”. Experience d’une maternite tunisienne // J. Gynecol. Obstet. Biol. Reprod. Paris, 1994, v. 23, no. 4, p. 451-455.
85. Block B.S., Mercer I.J., Ismail M.A. Clostridium difficile-associated diarrhea follows perioperative prophylaxis with cefoxitin // Am. J. Obstet. Gyn., 1985, v. 153, p. 835.
86. Bracero L.A. Ampicillin/sulbactam versus cefotetan for the prevention of infection following cesarean delivery in high-risk patients: a randomized double-blind trial. // Gynecol. obstet. Invest., Vol. 44, No. 1, 1997, p. 21-25.
87 Burke J.F. The effective period of preventive antibiotic action in experimental incisions and dermal lesions. // Surgery, 1961, v. 50, p. 161-168.
88. Burnakis T.G. Surgical antimicrobial prophylaxis: principles and guidelines. // Pharmacotherapy, V. 4, Sept.-Oct. 1984, p. 248-271.
89. Carlson C., Duff P. Antibiotic Prophylaxis for Cesarean Delivery: Is an Extended-Spectrum Agent Necessary? // obstet. Gynecol. Vol. 76, No. 3, part 1, Sept. 1990, p. 343-346.
90. Chang P.L., Newton E.R. Predictors of antibiotic prophylactic failure in post-cesarean endometrinis. // obstet. Gynecol., Vol. 80, no. 1, 1992, p. 117122.
91. Charles D., Edwards W.R. Infections complications of cervical cerclage. // Am. J. Obstet. Gynecol, 1981, v. 141, p. 1065-1071.
92. Chelmow D., Ruehli M.S., Huang E. Prophylactic use of antibiotics for nonlabouring patients undergoing cesarean delivery with intact membranes: a meta-analysis. // Am. J. Obstet. Gynecol., Vol. 184, No. 4, Mar. 2001, p. 656661.
93. Chia J.Y., Tan K.W., Tay L. A survey of postoperative wound infections in obstetrics and gynaecology // Singapore Med. J., 1993, v. 34, no. 3, p. 221224.
94. Currier J.S., Tosteson T.D., Piatt R. Cefazolin compared with cefoxitin for cesarean section prophylaxis: the use of two-stage stady design. // J. Clin. Epidemiol., 1993, July, v. 46, no. 7, p. 625-630.
95. Desjardins C., Diallo H.O., Audet-Lapointe P., Harel F. Retrospective study of post-cesarean endometritis // J. Gynecol. obstet. Biol. Reprod., 1996, v. 25, no. 4, p. 419-423.
96. Di Lieto A., Albano G., Cimmino E., Pontillo M., Gallo F., Micalef R., Paladini A. Studio retrospettivo della morbilita infettiva postoperatoria nel taglio cesareo. // Minerva Ginecol., 1996 March; 48(3), p. 85-92.
97. Dinsmoor M.J., Newton E.R., Gibbs R.S. A randomized, double-blind, placebo-controlled trial of oral antibiotic therapy following intravenous antibiotic therapy for post-partum endometritis // Obstet. Gynecol., 1991,v. 77, No. l, p. 60-62.
98. Duff P. Pathophysiology and management of postcesarean endometritis // Obstet. Gynecol., 1986, v. 67, no. 2, p. 269-276.
99. Ehrenkranz N.J., Blackwelder W.C. Infections complicating low-risk cesarean section in community hospitals: Efficacy of antimicrobial prophylaxis. // Am. J. Obstet. Gynecol. Vol. 162, No. 2,1990, p. 337-343.
100. Eschenbach D.A., Davick P.R., Willian B.L. et al. Prevalence of hydro-gen-peroxid-producing Lactobacillus species in normal women and women with bacterial vaginosis. // J. Clin. Microbiol., 1989, v. 27, p. 251-256.
101. Faro S. Antibiotic prophylaxis // Obstet. Gynecol. Clin. N. Amer., 1989, v. 16, no. 2, p. 279-289.
102. Faro S., Martens M.G., Hammil H., Riddle G., Tortolero G. Antibiotic prophylaxis: Is there a difference? // Am. J. Obstet. Gynecol., v. 162, No. 4, April 1990, p. 900-909.
103. Faro S., Phillips L.E., Martens M.G. Perspectives on the bacteriology of postoperative obstetric-gynecologic infections. // Am. J. Obstet. Gynecol., v. 158, No. 3, 1988, p. 694-700.
104. Fejgin M.D., Markov S., Goshen S., Segal J., Arbel Y., Lang R. Antibiotic for cesarean section: the case for ‘true’ prophylaxis. // Int. J. Gynaecol. Obstet., v. 43, No. 3, Dec. 1993, p. 257-261.
105. Figueroa Damian R., Ortiz Ibarra F.J., Labastida Dominguez V.M. et al. Ceftriaxona vs. cefazolina en la profilaxis quirurgica obstetrica. // Ginecol. obstet. Fur., 1995 Jul, 63, p. 302-307.
106. Gall S., Koukol D.H. Ampicillin/sulbactam vs clindamycin/gentamycin in the treatment of postpartum endometritis // J. Reprod. Med., 1996, v. 41, no. 8, p. 575-580.
107. Gibbs R. Infection after cesarean section // Clin. obst. Gyn., 1985, v. 28, no. 4, p. 697-710.
108. Gibbs R. A follow-up study on prophylactic antibiotics in cesarean section // Am. J. Obstet. Gynecol., 1972, v. 117, p. 419.
109. Gonik B., Shannon R.L., Shawar R., Costner M., Seibel M. Why patients fail antibiotic prophylaxis at cesarean delivery: histologic evidence for incipient infection. // obstet. Gynecol, v. 79, No. 2, Feb. 1992, p. 179-184.
110. Graham J.M., Blanco J.D., Oshiro B.T., Magee K.P., Monga M., Eriksen N. Single-dose ampicillin prophylaxis does not eradicate enterococcus from the lower genital tract. // obstet. Gynecol., v. 81, No. 1, Jan. 1993, p. 115-117.
111. Gugino L., Cimino M., Wactawski-Wende J. Single-dose antibiotics prophylaxis during cesarean section // Prim. Care Update Obstet. Gynecol., v. 5, No. 4, July 1998, p. 147-148.
112. Hemsell D.L. Prophylactic antibiotics in gynecologic and obstetric surgery // Rev. Infect. Dis., 1991, v. 13 (suppl. 10), s. 821-841.
113. Hillier S.L., Kiviat N.B., Hawes S.E. et al. Role of bacterial vaginosis-associated microorganisms in endometritis // Amer. J. Obstet. Gynecol., 1996, v. 175, no. 2, p. 435-441.
114. Huam S.H., Lim J.M., Raman S. Single dose antibiotic prophylaxis in women undergoing elective cesarean section. // Med. J.Malaysia, v. 52, No. 1, Mar. 1997, p. 3-7.
115. Huskins W.C., Ba-Thike K. et al. At international survey of practice variation in the use of antibiotic prophylaxis in cesarean section. // Int. J. Gyncol. obstet. v. 73, No. 2, May 2001, p. 141-145.
116. Itskowitz J., Paldi E., Katz M. The effect of prophylactic antibiotics on febrile morbidity following cesarean section. // obstet. Gynecol., 1979, v. 53, p. 162.
117. Jakobi P., Weissman A., Sigler E., Margolis K., Zimmer E.Z. Postcesarean section febrile morbidity. Antibiotic prophylaxis in low-risk patients. // J. Reprod. Med., v. 39, No. 9, Sep. 1994, p. 707-710.
118. Lang R., Shalit I., Segal J., Arbel Y „ Markov S., Hass H., Fejgin M. Maternal and fetal serum and tissue levels of ceftriaxone following preoperative prophylaxis in emergency cesarean section. // Chemotherapy, v. 39, No. 2, Mar-Apr. 1993, p. 77-81.
119. Litta P., Vita P., Konishi de Toffoli J., Onnis G.L. Risk factors for complicating infections after cesarean section. // clinic. Exp. obstet. Gynecol., v. 22, No. 1, 1995, p. 71-75.
120. Long W., Rudd E., Dillon M. Intrauterine irrigation with cefamandole nafale solution at cesarean section: a preliminary report // Am. J. Obstet. Gynecol, v. 138, no., 1980, p. 755-759.
121. McCoy M.C., Katz V.L., Kuller J.A. et al. Bacterial vaginosis in pregnancy: an approach for the 1990s. // obstet. Gynecol. Surv., 1995, v. 50, no. 6, p. 482-488.
122. McGregor J., Christiansen F. Treatment of obstetric and gynecologic infections with an emphasis on beta-lactamase-producing organisms // J. Re-prod. Med., 1988, v. 33, no. 6, suppl., p. 591-594.
123. Magann E.F., Washburne J.F. et al. Infectious morbidity, operative blood loss, and length of the operative procedure after cesarean delivery by method of placental removal and site of uterine repair.// J. Am. Coll. Surg., 1995, v. 181, p. 517-520.
124. Magee K.P., Blanco J.D., Graham J.M., Rayburn C., Prien S. Endometritis after cesarean: the effect of age. // Am. J. Perinatol., v. 11, No. 1, Jan. 1994, p. 24-26.
125. Mathelier A.C. // J. Reprod. Med., 1992, v. 20, no. 3, p. 177-182.
126. Naylor C.S., Steele L., Hsi R. et al. Cefotetan-induced hemolysis associated with antibiotic prophylaxis for cesarean delivery. // Am. J. Obstet. Gynecol. v. 182, No. 6, Jun. 2000, p. 1427-1428.
127. Newton E.R., Prihoda T., Gibbs R. A clinical and mycrobiologic analysis of risk factors for puerperal endometritis // Obstet. Gynecol. 1990, v. 75, No. 3, pt. l,p. 402-406.
128. Newton E.R., Wallace P.A. Effects of prophylactic antibiotics on endometrial flora in women with postcesarean endometritis. // obstet. Gynecol., v. 92, No. 2, 1998, p. 262-268.
129. Pedersen T.K., Blaakaer J. Antibiotic prophylaxis in cesarean section. // Acta Obstet. Gynecol. Scand., v. 75, No. 6, Jul. 1996, p. 537-539.
130. Peterson C.M., Medchill M. et al. Cesarean prophylaxis: a comparison of cefamandole and cefazolin by both intravenous and lavage routes, and risk factors associated with endometritis. // obstet. Gynecol., v. 75, No. 2, 1990, p. 179-182.
131. Pirwany I.R., Mahmood T. Audit of infective morbidity following cesarean section at a district general hospital. // J. Obstet. Gynaecol., v. 17, No. 5, 1997, p. 439-443.
132. Roca R., Nagy G., Redai I., Lampe L. Clinical significance of amniotic fluid bacteriological cultures taken at caesarean section. // clinic. Exp. obstet. Gynecol., v. 21, No. 2,1994, p. 99-102.
133. Rijhsinghani A., Savopoulos S.E. et al. Ampicillin/sulbactam versus am-picillin alone for cesarean section prophylaxis: a randomized double-blind trial. // Am. J. Perinat., v. 12, No. 5, Sept. 1995, p. 322-324.
134. Rehu M., Jahkola M. Prophylactic antibiotics in cesarean section: effect of a short pre-operative course of benzylpenicillin or clindamycin plus gen-tamicin on postoperative infections morbidity. // Ann. Clin. Res. 1980, no. 12, p. 45.
135. Rizk D. E., Nsanze H., Mabrouk M. H., Mustafa N., Thomas L., Kumar M. Systemic antibiotic prophylaxis in elective cesarean delivery.// Int. J. Gy-necol. Obstet. v. 61, No. 3, June 1998, p. 245-251.
136. Roberts S., Maccao M., Faro S. et al. The microbiology of post-cesarean wound morbidity // Obstet. Gynecol., 1993, v. 81, no. 3, p. 383-386.
137. Rouzi A.A., Khalifa F. et al. The routine use of cefasolin in cesarean section. // Infect. Dis. obstet. Gynecol., 2000, v. 69, no. 2, p. 107-112.
138. Smail F. Antibiotic prophylaxis and cesarean section. // Br. J. Obstet. Gynecol., v. 99 Oct. 1992, p. 789-790.
139. Soper D.E. Bacterial vaginosis and postoperative infections // Obstet. Gynecol., 1993, v. 169, No. 2, pt. 2, p. 467-469.
140. Soper D.E. Infections following caesarean section. // Curr. Opin. obstet. Gynecol, v. 5, No. 4, Aug. 1993, p. 517-520.
141. Spandorfer S.D., Graham E., Forouzan I. Postcesarean endometriis. Clinical risk factors predictive of positive blood cultures // J. Reprod. Med., 1996, v. 41, no. 11, p. 797-800.
142. Spinnato J.A., Youkilis B., Cook Y.D. et al. Antibiotic prophylaxis at cesarean delivery. // J. Matern. Fetal Med., v. 9, No. 6, Nov.-Dec. 2000, p. 348350.
143. Stovall T., Thorpe E., Ling F.W. Treatment of post-cesarean section endometritis with ampicillin and sulbactam or clindamycin and gentamicin. // J. Reprod. Med., v. 38, No. C, Nov. 1993, p. 843-848.
144. Sulovic V., Ljubic A., Cvetkovic M., Antonovic O., Pervulov M. Ceftriaxone in prevention of complications after cesarean section and its influence on the newborn. // clinic. Exp. obstet. Gynecol., Vol. 21, No. 1, 1994, p. 33-37.
145. Suonio S., Saarikoski S., Vohlonen I., Kauhanen O. // Int. J. Gynec. Obstet., 1989, v. 29, no. 2, p. 135-142.
146. Sweet R.L., Gibbs R.S. Infectious diseases of the female genital tract. // Baltimore, 3d. Ed., 1995, p. 729-745.
147. Walmer D., Walmer K., Gibbs R.S. Enterococci in post-cesarean endometritis // Obstet.