Etiquetas:
El moco cervical consiste en una sustancia mucosa secretada por las glándulas que se encuentran en el cuello uterino, influenciado directamente por los diferentes cambios hormonales a lo largo del ciclo reproductivo de la mujer, cambiando tanto la cantidad como su consistencia.
La función del moco cervical es imprescindible para evitar que cualquier sustancia extraña entre en el útero a través del cuello uterino. Y, además, nutre y ayuda a que los espermatozoides puedan alcanzar el útero a través del cuello uterino.
Lo cierto es que el moco cervical fértil se convierte en una pista tremendamente útil cuando la ovulación de acerca. De hecho, cuando se produce algún cambio en el moco cervical, y adquiere una textura y consistencia determinadas, muchas mujeres lo utilizan como una señal de fertilidad.
Así, el flujo vaginal es considerado como fértil cuando tiene una apariencia similar al que posee una clara de huevo cruda. Este es considerado uno de los mejores momentos para tener relaciones sexuales cuando se desea conseguir el embarazo.
Si bien es cierto que el moco cervical cambia a lo largo del ciclo menstrual de la mujer, cuando notas un flujo vaginal con una apariencia similar al que posee la clara de huevo, sería una señal de que se está a punto de ovular (es decir, significaría que la ovulación está cerca).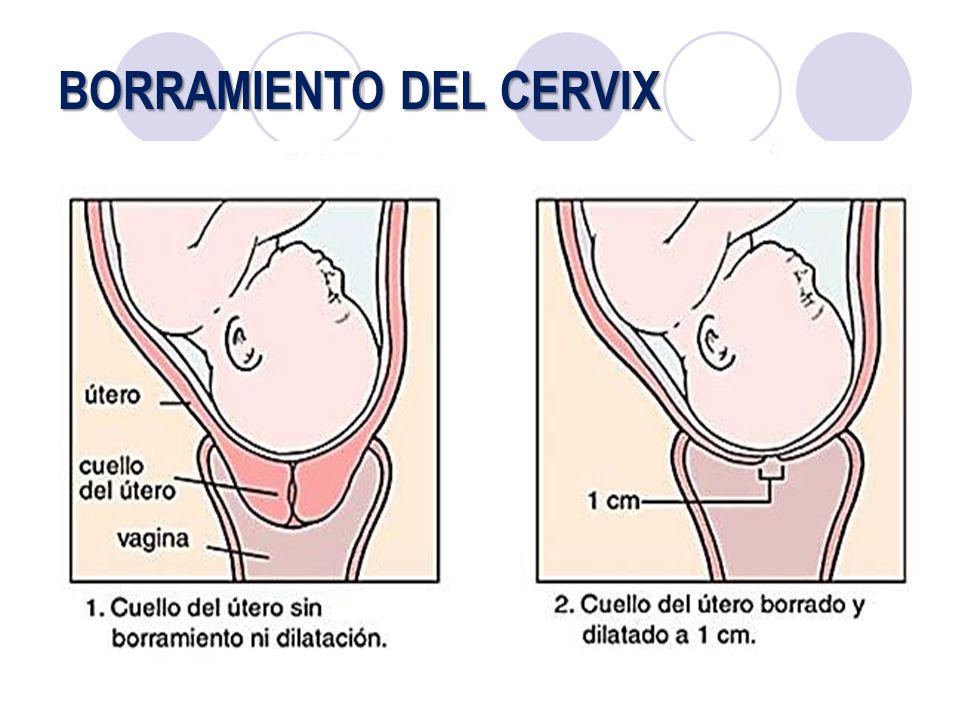 Es considerado, de hecho, el tipo de moco cervical más fértil.
Es considerado, de hecho, el tipo de moco cervical más fértil.
Esto es imprescindible, puesto que no siempre el flujo vaginal es del todo amigable con los espermatozoides. El moco cervical comienza después del período, y tiende a pasar de una consistencia pegajosa a una mucho más cremosa. Luego se vuelve acuosa, y finalmente, adquiere consistencia de clara de huevo cruda.
Una vez que la ovulación ha pasado, la progesterona hace que el moco cervical empiece a secarse, volviendo a adquirir una consistencia muchísimo más pegajosa y espesa, lo que impide que tanto los espermatozoides como cualquier otra sustancia extraña puedan llegar al útero.
Como veremos en el apartado próximo, la mujer por lo general obtendrá una secreción de clara de huevo fértil durante uno o dos días antes de ovular. Estos son considerados, precisamente, como los días de mayor fertilidad. Por lo que si se desea concebir, es imprescindible tener relaciones sexuales justo a partir del momento en el que el moco cervical adquiere esta consistencia.
Ovulación y moco cervical
Es decir, a medida que la ovulación se acerca, el moco cervical cambia de una consistencia en realidad no amigable a los espermatozoides, a una variedad muchísimo más fértil.
¿Y cuáles son las etapas por las que pasa el moco cervical a lo largo del ciclo menstrual?:
No obstante, la mayoría de expertos coinciden en señalar que, en realidad, existen cuatro tipos de moco cervical, que irían desde el tipo 1 (considerado como el menos fértil), hasta el tipo 4 (el más fértil).
A medida que el óvulo comienza a madurar, el cuerpo comienza a producir el conocido como “moco cervical tipo 3”. Se trata de una secreción más espesa, que adquiere una apariencia cremosa, y que se siente pegajosa entre los dedos. Esta sería considerada como una señal de que se estaría entrando en el período más fértil.
Ahora, mientras el cuerpo se prepara para la llegada de la ovulación, se produce una mayor cantidad de moco cervical. Así, cuando el moco cervical pasa a ser más fértil, tendrá una apariencia clara y una consistencia elástica, similar, como ya te hemos comentado en varias ocasiones, a las claras de huevo crudas. Además, tiende a estirarse unos pocos centímetros entre los dedos, y parecerá algo más transparente.
Por tanto, justo en este momento las probabilidades de quedarse embarazadas son, ahora, dos o tres veces más altas.
Después de la ovulación empezará a producirse una menor cantidad de moco cervical, sobre todo en los días previos al comienzo del período. Lo más habitual es que el moco se vuelva pegajoso y turbio. De hecho, el moco cervical no será fértil cuando no se estire mucho (o no lo haga en absoluto).
Lo más habitual es que el moco se vuelva pegajoso y turbio. De hecho, el moco cervical no será fértil cuando no se estire mucho (o no lo haga en absoluto).
En esta sección
Métodos de observación de la fertilidad
¿Qué es el método de la temperatura?
¿Qué es el método del moco cervical?
¿Qué es el método del ritmo?
¿Qué es el método de los días estándar?
¿Los métodos de observación de la fertilidad son lo indicado para mí?
El método del moco cervical es uno de los métodos de observación de la fertilidad. Te ayuda a predecir cuándo vas a ovular haciéndole seguimiento a los cambios en tu moco cervical (flujo vaginal) durante tu ciclo menstrual.
Te ayuda a predecir cuándo vas a ovular haciéndole seguimiento a los cambios en tu moco cervical (flujo vaginal) durante tu ciclo menstrual.
Las hormonas que controlan tu ciclo menstrual también hacen que el cuello uterino produzca el moco espeso y pegajoso que viene de tu cuello uterino. Este moco sale por tu vagina en forma de flujo (flujo vaginal). El moco cervical cambia de color, textura y cantidad durante tu ciclo menstrual, especialmente cuando estás cerca de la ovulación.
Para evitar el embarazo con el método del moco cervical, tienes que revisar tu moco todos los días y anotar los resultados en una tabla. Los cambios en tu moco te ayudan a saber cuándo vas a ovular, que es cuando estás fértil y puedes quedar en embarazo. Si deseas evitar embarazos, no tengas sexo vaginal o usa otro método anticonceptivo durante tus días días fértiles (peligrosos). En cambio, durante tus días infértiles (seguros) puedes tener relaciones vaginales sin protección.
El método del moco cervical también se conoce como método de la ovulación o método Billings. Es mejor comenzar a usar este método con la ayuda de alguien expertx, como unx doctorx, enfermerx o consejerx de planificación familiar, ya que puede ser difícil aprender a usarlo.
No uses el método del moco cervical como anticonceptivo hasta que le hayas hecho seguimiento a tu moco cervical durante al menos un (1) ciclo menstrual. El método del moco cervical es más efectivo cuando lo combinas con el método de la temperatura.
Hay otro método del moco cervical que se llama método de 2 días.
Debes tocar y observar tu moco (o flujo) todos los días y registrar lo que notes en una tabla especial. Puedes comenzar a hacerle seguimiento a tu moco cervical el día después de que tu periodo termine completamente.
Puedes revisar tu moco cervical de 3 maneras:
Limpia la abertura de tu vagina con papel higiénico o un pañuelo de papel ANTES de orinar (hacer pipí). Revisa el color y siente la textura del moco.
Revisa el color y siente la textura del moco.
Observa el color y la textura del flujo en tu ropa interior.
Introduce tus dedos limpios en la vagina y después observa el color y la textura del moco en tus dedos.
La mejor manera de sentir la consistencia del moco es frotarlo y extenderlo entre tu dedo pulgar e índice. Anota todo lo que veas acerca de tu moco cervical en una tabla todos los días: los días de tu periodo, los días secos, los días húmedos, los días pegajosos, los días turbios y los días resbalosos.
Cuando comienzas a hacerle seguimiento a tu moco cervical, es mejor evitar el sexo vaginal durante un (1) ciclo completo o usar condón. El sexo puede hacer que tu cuerpo produzca más moco o que tu moco cambie, lo que puede ser confuso cuando estás comenzando.
Tu moco cervical cambia a lo largo del mes, dependiendo de en qué momento de tu ciclo menstrual te encuentres:
Durante tu periodo: la sangre menstrual hace que no puedas ver tu moco. Los días cuando te baja el periodo son días peligrosos (fértiles).
Los días cuando te baja el periodo son días peligrosos (fértiles).
Cuando tu periodo termina: justo después de que tu periodo termina, usualmente tienes 3 o 4 días sin moco ni flujo. Se llaman “días secos” y si tu ciclo menstrual es largo, pueden ser días seguros (infértiles).
Antes de la ovulación: tu cuerpo produce más moco justo antes de la ovulación, cuando el óvulo comienza a madurar. Este moco suele ser amarillo, blanco o turbio, y tiene una textura pegajosa o viscosa. Lo puedes notar en la abertura de tu vagina durante 3 a 5 días. Estos días son menos seguros.
Justo antes y durante la ovulación: usualmente es cuando tienes más cantidad de moco cervical. El moco es claro y tiene una textura resbalosa, parecida a la clara de huevo cruda. Además, lo puedes estirar entre tus dedos. Estos “días resbaladizos” son tus días peligrosos (fértiles), cuando tienes más chances de quedar en embarazo. Duran aproximadamente 4 días y van desde antes de la ovulación hasta cuando esta termina.
Duran aproximadamente 4 días y van desde antes de la ovulación hasta cuando esta termina.
Después de la ovulación: puede que tengas menos moco de repente. Además tu moco se vuelve turbio y pegajoso nuevamente, y después tienes algunos días secos (sin moco). Esto dura más o menos entre 11 y 14 días que son seguros (infértiles).
Después te baja el periodo y se repite el ciclo menstrual.
Los días seguros (infértiles) y los días peligrosos (fértiles) varían de persona a persona, dependiendo de la duración del ciclo menstrual. Durante tus días seguros, puedes tener sexo vaginal sin protección. Durante tus días peligrosos (fértiles), no tengas sexo vaginal o si lo haces, usa otro método anticonceptivo.
Días seguros
En general, tienes una fase principal de tu ciclo con días infértiles o seguros: tus días seguros comienzan después de la ovulación, cuando desaparece el moco más resbaladizo y tu flujo vuelve a ser turbio y pegajoso, y después desaparece (días secos), justo antes de tu periodo.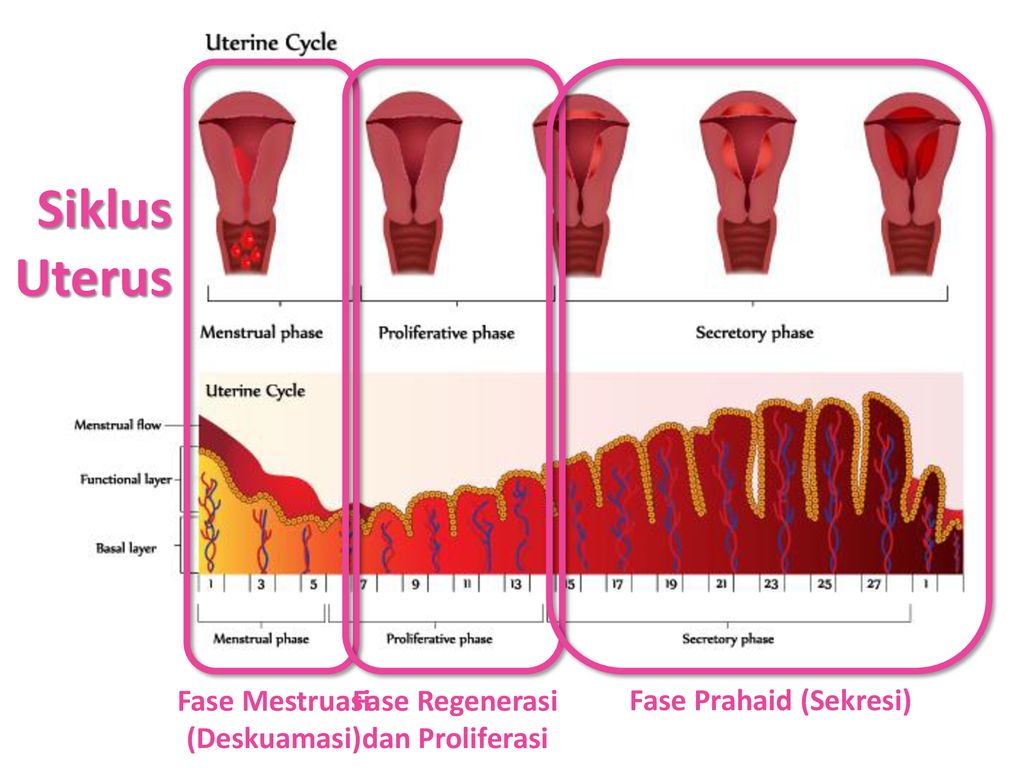 Esto dura entre 11 y 14 días en promedio (puedes leer más arriba donde dice “después de tu periodo”).
Esto dura entre 11 y 14 días en promedio (puedes leer más arriba donde dice “después de tu periodo”).
Si tienes un ciclo menstrual largo, los días secos justo después de que tu periodo desaparece también son días seguros.
Días peligrosos
En un ciclo menstrual promedio hay tres fases principales de días peligrosos o fértiles:
Los días donde tienes tu periodo son peligrosos, sobre todo si tienes un ciclo menstrual corto. Esto es así porque cuando tienes el periodo, no puedes saber cómo se ve tu moco cervical o cuál es su textura, pues está mezclado con la sangre menstrual.
La otra fase del ciclo con días peligrosos empieza unos días después de que termina tu periodo, pero 2 o 3 días antes de que tienes las primeras señales del moco resbaladizo, que es mientras tu cuerpo está haciendo el moco pegajoso y viscoso (turbio). Quizá notes este flujo en la apertura de tu vagina durante 3 a 5 días. Estos días son menos seguros.
Los días peligrosos o fértiles continúan mientras tu cuerpo produce moco resbaladizo antes de la ovulación. Estos días peligrosos duran más o menos 3 a 4 días, y terminan aproximadamente 4 días despues de que el moco resbaladizo llega a su punto máximo.
Algunas actividades o condiciones pueden hacer que el moco cervical natural cambie. En estos casos el método del moco cervical es menos efectivo y más difícil de usar.
Algunas de las actividades y condiciones que pueden afectar el moco cervical son:
el sexo vaginal
usar lubricante (ya sea para el sexo o durante un examen pélvico)
usar algunos medicamentos
La lactancia (amamantar)
la cirugía de cuello uterino
las duchas vaginales
la menopausia prematura
haber usado anticonceptivos hormonales recientemente (incluyendo la pastilla del día después)
las enfermedades de transmisión sexual (ETS)
la vaginitis
Los métodos del moco cervical no son una buena opción para las personas que no tienen mucho flujo. Si utilizas este método para evitar el embarazo y tienes preguntas acerca de tu moco cervical, habla con tu doctorx..
Si utilizas este método para evitar el embarazo y tienes preguntas acerca de tu moco cervical, habla con tu doctorx..
El método de dos días también es un método del moco cervical pero más sencillo. Funciona mejor cuando tu cuerpo produce suficiente moco como para poder hacerle seguimiento todos los días y saber si tienes moco o no.
El método de dos días es fácil de usar. Para tener una idea, responde las siguientes preguntas:
Si tu respuesta a AMBAS preguntas es no, es seguro tener sexo vaginal. Si tu respuesta a CUALQUIERA de las dos preguntas es sí, utiliza otro método anticonceptivo o evita tener sexo vaginal.
Puede que las personas que usan este método solo tengan 12 días seguros (infértiles) durante cada ciclo menstrual.
En realidad no importa en qué momento del día revises tu moco cervical. Sin embargo es muy importante que lo cheques todos los días. A diferencia del método de la temperatura (también conocido como método de la temperatura basal), no necesitas revisar tu moco cervical a primera hora de la mañana. Lo importante es que seas constante y lo revises todos los días, sin falta.
A diferencia del método de la temperatura (también conocido como método de la temperatura basal), no necesitas revisar tu moco cervical a primera hora de la mañana. Lo importante es que seas constante y lo revises todos los días, sin falta.
The structure of the cervix
The cervix is a part of the uterus, which at one end is partially located in the vagina, and at the other through the internal pharynx passes into the cavity of the uterine body.
It has the shape of a cylinder with a channel inside. Through the outer hole, the so-called. external os, the cervical canal opens into the vagina. Through the inner hole, the so-called. internal os, the cervical canal opens and connects with the uterine cavity. The overall dimensions of the cervix can vary from 2-3 cm to 4-6 cm, both in length and in diameter. nine0005
Fig.1 . Schematic representation of the internal genitalia
The cervix is a muscular-connective tissue organ, which is covered with epithelial tissue. In the connective tissue are blood and lymphatic vessels, muscle tissue is represented by smooth muscles. The main part of the muscle tissue is located in the upper part of the cervix in the form of a ring and performs a locking function. Closer to the vaginal part, the cervix contains mostly connective tissue fibers. Epithelial tissue covers the cervix from the vaginal part and inside the cervical canal. nine0005
In the connective tissue are blood and lymphatic vessels, muscle tissue is represented by smooth muscles. The main part of the muscle tissue is located in the upper part of the cervix in the form of a ring and performs a locking function. Closer to the vaginal part, the cervix contains mostly connective tissue fibers. Epithelial tissue covers the cervix from the vaginal part and inside the cervical canal. nine0005
The part of the cervix that is located in the vagina and is visible to the doctor during examination is called the ectocervix. This part of the cervix has a smooth surface, covered with stratified squamous non-keratinized epithelium, the same as the vagina, and the mucous membrane of the labia minora.
Fig.2 . Microphotogram of normal stratified squamous epithelium. The microphotogram was kindly provided by Mikhail Krotevich, Candidate of Medical Sciences, Head of the Department of Pathology of the National Cancer Institute
This epithelium is smooth, pink, resistant to mechanical stress and the acidic environment of the vagina.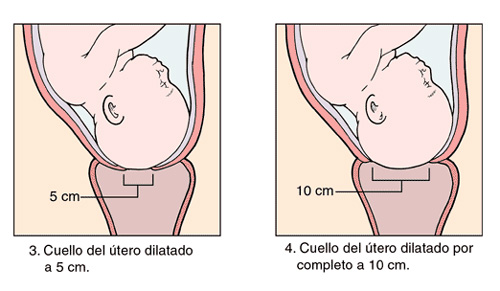 Stratified squamous epithelium performs a protective function. It is quickly updated and restored in case of mechanical injuries. Complete renewal of the epithelial layer occurs in 4-5 days.
Stratified squamous epithelium performs a protective function. It is quickly updated and restored in case of mechanical injuries. Complete renewal of the epithelial layer occurs in 4-5 days.
Fig.3 . On the colpophotogram, the cervix is covered with normal stratified squamous epithelium.
In the cervical canal the mucous membrane has a folded shape, is represented by multiple bends of the connective tissue, which resemble glands, is covered with a single layer of delicate epithelium – columnar epithelium. This epithelium produces clear mucus. Mucus in the cervical canal forms a mucous plug. The nature and type of cervical mucus changes with the phases of the menstrual cycle. In the first phase of the mucus cycle, there is a little more; during ovulation, it becomes transparent and viscous. nine0005
Stratified squamous epithelium and columnar epithelium meet at the external os and form a junction line.
Fig.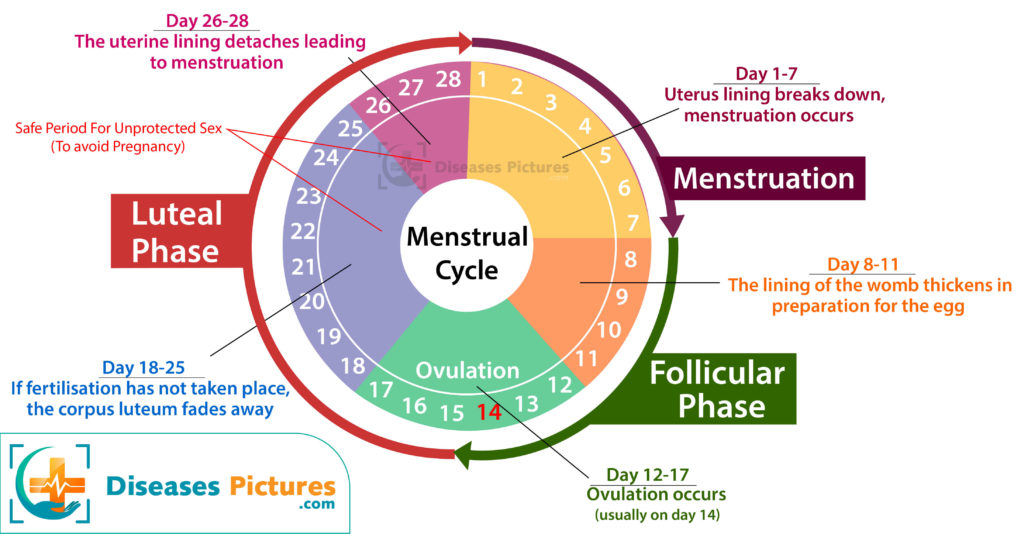 4 . The colpophotogram shows the cervix during ovulation. In the cervical canal, there is transparent mucus, the mucous membrane of the cervical canal is visible, the junction line of two types of epithelium at the level of the external os.
4 . The colpophotogram shows the cervix during ovulation. In the cervical canal, there is transparent mucus, the mucous membrane of the cervical canal is visible, the junction line of two types of epithelium at the level of the external os.
The joint is necessary and desirable to be visualized during colposcopy, and it must necessarily fall into the area of taking a cytological smear (Pap test). nine0005
Why is this important?
It is known that the main cause of dysplasia and cervical cancer is the human papillomavirus. This virus can only replicate in actively dividing cells. Such cells are found in the stratified squamous epithelium in its lowest layers – basal cells. However, with the preserved integrity of the epithelium, they are reliably protected by the upper layers. The only “weak” place on the cervix, where the virus can “get” to such cells, is the junction. nine0005
Fig. 5 . Schematic representation of the junction of stratified squamous epithelium and cylindrical.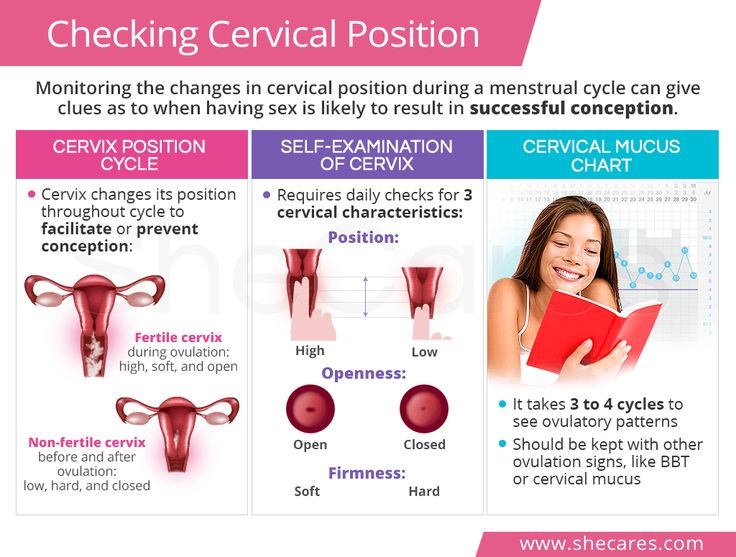 It is clearly seen that the basal cells at the junction are located close to the surface – this is the “weak link”.
It is clearly seen that the basal cells at the junction are located close to the surface – this is the “weak link”.
There, the lower (basal) cells rise to the surface and remain vulnerable to the virus. As a rule, all pathological processes in the epithelium of the cervix begin to occur in the junction area, so it is important to have a mandatory colposcopic and cytological examination of this area of the cervix. nine0005
The third normal type of cervical epithelium is the metaplastic epithelium. The word “metaplasia” scares patients somewhat, because it is somewhat consonant with the word “metastasis”, but it has nothing to do with it.
Fig. 6 . The colpogram shows the cervix with a small ectopia of the cylindrical epithelium and a type 1 transformation zone of the cervix (metaplastic epithelium and multiple open glands), the junction is clearly visible, which is located on the outer part of the cervix – the ectocervix. nine0005
Metaplastic epithelium arises from reserve cells, the so-called. bipotent cells, or in other words, cells that have two possibilities for development. These cells are able, depending on the conditions, to transform either into cells of a cylindrical or into cells of a stratified squamous non-keratinized epithelium through the process of metaplasia. The process of metaplasia is stepwise. Metaplasia is early, immature and mature. In terms of properties and appearance, early metaplasia cells are similar to cells of a cylindrical epithelium; very early metaplasia can sometimes imitate a malignant process for an inexperienced morphologist (histologist or cytologist). According to the degree of maturation, metaplasia acquires the properties of a stratified squamous epithelium. If nothing interferes with the process of metaplasia (trauma, inflammation, infection with HPV), then it ends with the formation of a stratified squamous non-keratinizing epithelium. The process of metaplasia occurs on the cervix in the presence of ectopia on it columnar epithelium , as well as in the process of healing epithelial defects – erosion and abrasions, injuries.
bipotent cells, or in other words, cells that have two possibilities for development. These cells are able, depending on the conditions, to transform either into cells of a cylindrical or into cells of a stratified squamous non-keratinized epithelium through the process of metaplasia. The process of metaplasia is stepwise. Metaplasia is early, immature and mature. In terms of properties and appearance, early metaplasia cells are similar to cells of a cylindrical epithelium; very early metaplasia can sometimes imitate a malignant process for an inexperienced morphologist (histologist or cytologist). According to the degree of maturation, metaplasia acquires the properties of a stratified squamous epithelium. If nothing interferes with the process of metaplasia (trauma, inflammation, infection with HPV), then it ends with the formation of a stratified squamous non-keratinizing epithelium. The process of metaplasia occurs on the cervix in the presence of ectopia on it columnar epithelium , as well as in the process of healing epithelial defects – erosion and abrasions, injuries.
The entire surface area of the cervix, on which metaplasia occurs, is called the transformation zone of the cervix (restructuring zone, Fig. 6, 7). This is the place where the processes of transformation of the epithelium are actively taking place, and these areas of the cervix are very sensitive to the negative effects of the human papillomavirus.
Fig.7 . Microphotogram. Transformation zone of the cervix under the microscope: stratified squamous epithelium, columnar epithelium, metaplastic epithelium, junction line. The microphotogram was kindly provided by Mikhail Krotevich, Candidate of Medical Sciences, Head of the Department of Pathology of the National Cancer Institute. nine0005
It is very important to examine this area colposcopically and cytologically, since the risk of developing precancer and cervical cancer is many hundreds of times higher in it than in stratified squamous epithelium outside this area.
Transformation zones of the cervix are divided into three types:
Fig. 8 . Transformation zone type 1 is located on the outer part of the cervix and is fully visible during colposcopy;
8 . Transformation zone type 1 is located on the outer part of the cervix and is fully visible during colposcopy;
Fig. 9 . Transformation zone type 2 is located on the outer part of the cervix, but also has a component located in the cervical canal, but is completely visible; nine0005
Fig. 10 . The type 3 transformation zone has an intracervical component and is not completely visible.
Author of the article:
Bataeva Roza Saidovna
The chief doctor of the Center for Fruit medicine in Moscow, a specialist in prenatal diagnosis (medicine of the fetus), an ultrasonic diagnosis, candidate of medical sciences.
Contents
Miscarriage is a serious problem in modern obstetrics. About 10-20% of pregnancies end in spontaneous miscarriages or premature births. There are many possible reasons for miscarriage. These are hormonal disorders, and mother’s diseases, and genetic disorders, and the impact of environmental factors. One of the serious problems leading to miscarriage is the so-called isthmic-cervical insufficiency .
About 10-20% of pregnancies end in spontaneous miscarriages or premature births. There are many possible reasons for miscarriage. These are hormonal disorders, and mother’s diseases, and genetic disorders, and the impact of environmental factors. One of the serious problems leading to miscarriage is the so-called isthmic-cervical insufficiency .
The uterus is shaped like a pear. In its structure, the body and neck are distinguished. During pregnancy, the fetus is located inside the body of the uterus, and due to the presence of muscle cells, the body of the uterus increases significantly during pregnancy. The cervix has the shape of a cylinder. From the side of the body of the uterus, it is limited by the internal pharynx, in the area of \u200b\u200bwhich, in addition to muscle cells, there is a large amount of connective tissue, and a ring is formed that helps to keep the fetus in the uterus (sphincter). The area where the body of the uterus passes into the cervix is called the isthmus. In the vagina, the cervix opens with an external os. During childbirth, there is a smoothing of the cervix, relaxation of muscle cells and opening of the cervix, which forms the birth canal. nine0005
In the vagina, the cervix opens with an external os. During childbirth, there is a smoothing of the cervix, relaxation of muscle cells and opening of the cervix, which forms the birth canal. nine0005
In violation of the integrity or function of the sphincter and the internal os of the cervix, insufficient closing function of the isthmus, the so-called isthmic-cervical insufficiency develops.
With isthmic-cervical insufficiency during pregnancy, spontaneous smoothing and opening of the cervix occurs, not associated with the contractile activity of the uterus. At the same time, the fetal egg loses the necessary support in the lower uterine segment. With increasing pressure inside the uterus, the membranes begin to protrude into the dilated cervical canal, which leads to premature birth. Usually childbirth begins with premature rupture of amniotic fluid. This is because the fetal membranes protruding into the cervical canal can become infected with bacteria that are part of the vaginal microflora. As a result, the membranes lose their elasticity, they spontaneously break, the amniotic fluid is poured out and the baby is infected in utero with bacteria in the pregnant woman’s vagina. nine0005
As a result, the membranes lose their elasticity, they spontaneously break, the amniotic fluid is poured out and the baby is infected in utero with bacteria in the pregnant woman’s vagina. nine0005
First of all, these are previous injuries. They lead to the so-called traumatic or organic ICI. Most often, these are traumatic births, in which the cervix ruptures, previous abortions or diagnostic curettage of the uterine cavity, during which an instrumental dilation of the cervix is performed. In this case, a violation of the integrity of the isthmic ring of the neck and the formation of coarse scar tissue at the site of injury is possible. nine0005
Functional isthmic-cervical insufficiency is formed as a result of hormonal disorders in the body of a pregnant woman. This can be a pronounced underdevelopment of the internal genital organs, a deficiency of sex hormones, a decrease in the normal function of the ovaries, sometimes ICI is formed with an increased level of male sex hormones in the blood. All of these reasons lead to a violation of the ratio of muscle and connective tissue in the isthmus and cervix, the reaction of muscle cells of the cervix to nerve impulses changes. nine0005
All of these reasons lead to a violation of the ratio of muscle and connective tissue in the isthmus and cervix, the reaction of muscle cells of the cervix to nerve impulses changes. nine0005
In rare cases, with malformations of the uterus, congenital isthmic-cervical insufficiency may occur.
There are no specific symptoms of isthmic-cervical insufficiency. A pregnant woman may be disturbed by heaviness in the lower abdomen or in the lumbar region, the urge to urinate may become more frequent due to the pressure of the fetus on the bladder. However, most often the expectant mother is not worried about anything. nine0005
The diagnosis of isthmic-cervical insufficiency is made mainly during pregnancy, since only during pregnancy there are objective conditions for assessing the function of the cervix and its isthmic department. Outside of pregnancy, doctors take a number of special tests to detect CCI. An X-ray examination of the uterus is carried out on the 18-20th day of the cycle, an assessment is made of the degree of expansion of the cervical canal in the second phase of the menstrual cycle using special tools. nine0005
An X-ray examination of the uterus is carried out on the 18-20th day of the cycle, an assessment is made of the degree of expansion of the cervical canal in the second phase of the menstrual cycle using special tools. nine0005
During pregnancy, transvaginal ultrasound is used to monitor the cervix . This measures the length of the cervix. The length of the cervix less than 3 cm at a gestational age of less than 20 weeks requires the inclusion of a woman in a high-risk group for CI and careful monitoring of such a patient.
In women carrying twins or triplets up to 28 weeks of gestation, a cervical length of more than 37 mm in primigravidas and more than 45 mm in recurrent patients is considered normal. In multiparous women, the length of the cervix in the period of 17-20 weeks of pregnancy should be more than 29mm.
The absolute sign of isthmic-cervical insufficiency is the shortening of the cervix up to 2 cm and less . The measurement of the length of the cervix is influenced by various factors – for example, the tone of the uterus and the height of the placenta. In addition, it is important how the ultrasound doctor evaluates the length of the cervix. The most correct results are obtained with transvaginal (that is, examination with a sensor inserted into the patient’s vagina) access. This method of examining the cervix is absolutely safe for the further course of pregnancy and cannot cause a threat of interruption or other complications. nine0005
In addition, it is important how the ultrasound doctor evaluates the length of the cervix. The most correct results are obtained with transvaginal (that is, examination with a sensor inserted into the patient’s vagina) access. This method of examining the cervix is absolutely safe for the further course of pregnancy and cannot cause a threat of interruption or other complications. nine0005
When examining the cervix through the abdominal wall, that is, transabdominally, measurements of the length of the cervix are about half a centimeter higher than those during transvaginal examination, in addition, the degree of filling of the bladder affects the change in its length. In addition to the length of the cervix, during an ultrasound examination, the state of the internal pharynx is assessed, whether there is an opening of the pharynx and a bulging of the fetal bladder into the cervical canal.
However, it is not correct to make a diagnosis of isthmic-cervical insufficiency only on the results of an ultrasound examination. More accurate information is provided by an examination of the cervix by a gynecologist. Examination is performed in a gynecological chair. In this case, the doctor evaluates the length of the vaginal part of the cervix, its density, the degree of opening of the cervical canal. nine0005
More accurate information is provided by an examination of the cervix by a gynecologist. Examination is performed in a gynecological chair. In this case, the doctor evaluates the length of the vaginal part of the cervix, its density, the degree of opening of the cervical canal. nine0005
Learn more about services:
In order to prevent premature birth in isthmic-cervical insufficiency, from 20 to 34 weeks of pregnancy, progesterone preparations (DUFASTON, UTROZHESTAN) are prescribed – a hormone produced in the placenta and supporting pregnancy.
There are two ways to treat cervical insufficiency. These are non-surgical methods and surgical. nine0005
Non-surgical methods include the insertion into the vagina of special obstetric pessaries – rings that are put on the cervix and prevent its further opening, supporting the presenting part of the fetus. Non-surgical methods have a number of advantages – they do not require hospitalization, anesthesia and are easy to use. Pessaries are usually used after 28 weeks of pregnancy. Before the introduction of the ring, a smear must be taken on the flora to identify and treat a possible inflammatory process. After the introduction of an obstetric pessary, it is necessary to treat the vagina and the ring with antiseptic solutions every 2-3 weeks to prevent the development of infection. However, this method may not always be applicable. nine0005
Non-surgical methods have a number of advantages – they do not require hospitalization, anesthesia and are easy to use. Pessaries are usually used after 28 weeks of pregnancy. Before the introduction of the ring, a smear must be taken on the flora to identify and treat a possible inflammatory process. After the introduction of an obstetric pessary, it is necessary to treat the vagina and the ring with antiseptic solutions every 2-3 weeks to prevent the development of infection. However, this method may not always be applicable. nine0005
With severe isthmic-cervical insufficiency, the use of rings is ineffective. They are also not used when the fetal bladder bulges into the cervical canal. In these cases, treatment is carried out by suturing the cervix.
Indications for surgical correction of ICI:
 nine0124
nine0124 Contraindications for surgical treatment:
Cervical suturing is usually done between 13 and 27 weeks of pregnancy. The timing of the operation is determined individually by the attending physician. The most favorable period for surgical treatment is from 15 to 19week of pregnancy, when the opening of the cervix is not very pronounced and the fetal bladder does not swell into the canal.
The cervix is sutured under general anesthesia. In some cases, for example, when the lower pole of the fetal egg bulges into the cervical canal, after surgery, in order to prevent possible infection of the membranes, a course of antibiotics is prescribed.